
本指南中使用的缩写和符号
执行摘要
建议摘要
严重疾病需要高水平的补充氧气
如果患者是低氧血症,需要中等水平的补充氧气的严重疾病
应密切监测患者的条件,但除非患者是低氧血症,否则不需要氧疗
COPD和其他需要控制或低剂量氧疗的病症
用于床边图表的氧气设备的缩写。
图1-医院急性低氧血症患者的氧气处方指导
图2 - 医院普通病房的氧气管理流程图
第1节简介
指南的目标
指南的目标用户和目标患者群体
指南涵盖的领域
指南未涵盖的领域
自2008年指南以来的变化摘要
指南的局限性
第2节指南制作的方法
建立指南团队
关键问题摘要
证据如何被纳入指南
试行,实施和审计指南
计划审查和更新指南
感兴趣的声明
签署证据水平
SIGN评级等级
第3节正常值和定义
健康和疾病中的氧气和二氧化碳的血气水平
正常范围为氧饱和度(SaO2和血氧饱和度2)和PO 2(PAO 2)血液中的在海平面
老年人的氧饱和度
高海拔氧饱和度
急性和慢性疾病的氧饱和度
睡眠期间氧饱和度的变化
动脉二氧化碳张力的正常范围
低氧血症,缺氧,1型呼吸衰竭和高氧血症的定义
高碳酸血症和2型呼吸衰竭的定义
酸中毒的定义(呼吸性酸中毒和代谢性酸中毒)
平均值(SD)PaO 2(kPa和mmHg)和SaO 2(%)值(范围)
Spo 2的范围,平均值,SD,中位数和IQR值(%),其中对患者接受来自Smith 等人年龄≥18岁(n = 37 299)的空气进行测量
第4节一般血气生理学
氧气生理学
二氧化碳生理学
目标氧饱和度(SaO 2)范围的概念
第5节高级血气生理学和氧疗的病理生理学和生理学
调节血氧含量(CaO 2)
动脉血氧分压
分血器
氧合血红蛋白解离曲线和玻尔效应
DO 2的监管
缺氧和高氧的病理生理学
低氧血症
其他缺氧机制
高氧
二氧化碳的生理学
正常二氧化碳稳态
调节二氧化碳
高碳酸血症和低碳酸血症的病理生理学
高碳酸血症和低碳酸血症的机制
通气不足和过度通气
氧疗的生理学
改善氧合和分娩的策略
优化PaO 2
优化氧气运输
优化交付
CaO 2的调节
对低氧血症的通气反应
氧离解曲线与玻尔效应
总二氧化碳解离曲线
PaCO的影响2
SaO 2和PaO 2之间的近似关系
第6节缺氧,低氧血症,高氧血症,高碳酸血症和靶向氧疗的理由
缺氧/低氧血症的影响和风险以及目标氧饱和度范围的基本原理
在急性疾病中,理想的氧饱和度范围
非低氧血症患者的高氧血症和补充氧疗的潜在益处
已经证明高氧血症在以下情况下是有益的
非低氧血症患者的其他潜在益处和氧疗的潜在危害
补充氧疗和高氧血症的潜在不良生理影响和临床风险
呼吸系统
突然停止补充氧疗后出现反应性低氧血症
心血管和脑血管系统
活性氧,组织毒性和死亡率增加的报告
延迟识别生理恶化
急性百草枯中毒,博莱霉素肺损伤和酸吸入急性肺损伤
高氧血症和补充氧疗的风险综述
高碳酸血症(和呼吸性酸中毒)的风险
血液二氧化碳水平升高的影响
临床症状
酸中毒的风险
氧疗的基本原理
急性疾病的目标氧饱和度
身体定位的影响包括约束系统
急性低氧血症和高氧血症的生理影响
第7节低氧血症和高碳酸血症的临床和实验室评估
评估低氧血症
呼吸困难患者的临床评估和紫绀的评估
价值和限制脉搏血氧仪
动脉和动脉血气
经皮氧评估
评估高碳酸血症和酸中毒
临床评估
血液动脉和小动脉气体
静脉PCO 2采样
二氧化碳监测和高碳酸血症的非侵入性评估
第8节医院和医疗机构的紧急氧气使用
到达医院时呼吸困难患者的评估和即时管理
与院前环境相比,医院管理方面的差异
哪些患者需要氧疗?
哪些患者需要血气测量?
动脉化的耳垂气体可以用作ABG的替代物吗?
氧气应以固定浓度处方还是达到目标饱和度?
接受补充氧气的患者的目标氧饱和度范围应该是多少?
大多数患者的氧饱和度目标范围
特定患者群体的氧气需求量
血气测量在指导氧疗中的重要性
什么应该是医院环境中氧气输送系统的最初选择?
用于医院紧急氧疗的装置
推荐用于治疗重大医疗急症和重症的氧疗
心脏骤停和其他需要心肺复苏的病症
重症患者包括严重创伤,休克和严重败血症
溺死
过敏性反应
主要肺出血或大量咯血
癫痫发作
主要头部受伤
一氧化碳中毒
如果患者是低氧血症,需要中等水平的补充氧气的严重疾病
原因不明的低氧血症患者,既往无呼吸系统疾病或危险因素
急性哮喘
肺炎
肺癌和肺部受累的其他癌症
纤维化肺病和其他涉及实质性肺病或肺泡炎的病症的恶化
气胸
胸腔积液
肺栓塞
急性心力衰竭
严重贫血引起的呼吸急促
镰状细胞危机
对于可能易受中等或高浓度氧气影响的患者,推荐使用氧气疗法
COPD恶化
CF的恶化
慢性肌肉骨骼和神经系统疾病
肥胖 - 通气不足综合症
常见的医疗紧急情况,只有在存在低氧血症时才需要进行氧疗
急性心肌梗死,疑似心肌梗死和急性冠状动脉综合征
行程
焦虑和过度通气或呼吸功能障碍
中毒除一氧化碳或氰化物以外的物质
代谢,内分泌和肾脏疾病
急性和亚急性神经肌肉疾病导致呼吸肌无力
集群头痛
产科紧急情况和劳动力
在术后和围手术期护理中使用氧气,包括使用PCA装置
氧气使用,脉搏血氧饱和度和术后低氧血症的发生率
患者自控镇痛
高氧血症在减少术后并发症中的作用
在内窥镜检查和其他涉及清醒镇静的程序中使用氧气
在姑息治疗环境中使用氧气
使用氦氧混合物(Heliox)
使用CPAP
在围手术期护理中使用CPAP
CPAP在急性肺水肿中的应用
第9节在救护车,社区和院前环境中使用氧气
脉搏血氧饱和度和氧气的可用性
第一响应者(全科医生,护士或救护人员)的临床评估
立即管理低氧血症患者
患有已知COPD的患者
应该假设患有COPD的患者
其他患有高碳酸血症呼吸衰竭伴呼吸性酸中毒的患者
COPD患者(以及其他有呼吸系统酸中毒风险的患者)发生高碳酸血症呼吸衰竭的氧气警报护理和24%或28%文丘里面罩
在院前护理中选择设备
在患者家中紧急使用氧气
救援和其他非NHS急救人员使用氧气
使用氧化亚氮/氧气混合物(例如,Entonox)
在孕前服用孕妇使用氧气
氧气警报卡的示例
第10节氧疗的实用方面
储氧和供应以及安全
气瓶
液氧
氧气浓缩器
患者分娩方法/接口
高浓度水库面罩(非再呼吸面罩)
简单的面膜
文丘里面具
鼻导管
通过鼻插管的高流量加湿氧气
气管切开术面罩
无创通气
在救护车中患者运输期间的氧气运输和运送
健康与安全执行氧气瓶安全使用指南
英国救护车服务使用氧气
其他车辆以及初级保健机构和患者家中的氧气运输
私家车中的氧气运输(健康与安全执行指导)
医疗中心和初级保健实践
在患者家中紧急使用氧气
医院的氧气输送系统
围手术期和术后护理
急诊科
普通病房和呼吸科
用于紧急氧疗的装置
流量计
氧气管和氧气壁出口
使用加湿氧气
合理使用加湿氧气
使用气泡加湿系统
大容量雾化加湿器
气管造口术或喉切除术患者使用氧气
为需要雾化支气管扩张剂治疗的患者提供氧气
雾化吸入支气管扩张剂治疗哮喘
雾化支气管扩张剂治疗COPD患者和其他高碳酸血症呼吸衰竭的危险因素
氦氧混合物(Heliox)的交付
氧化亚氮/氧气混合物的输送(例如,Entonox)
在可能部分阻塞气道的过程中输送氧气
CPAP设备和适应症
常见氧气瓶尺寸和容量的示例
文丘里面罩的总气体流量
高浓度水库面具
简单的面膜
文丘里面罩,浓度范围,文丘里面罩的操作
B文丘里面罩的建议流量和高呼吸率的调整
氧饱和度对治疗的反应
鼻导管
高流量加湿鼻导管,流量发生器和加湿器系统
气管切开术面罩
流量计
出风口盖
大容量雾化加湿器
第11节氧疗的处方,管理和监测
安全处方和氧气管理
医用氧气的法律地位:是否需要处方?
开氧疗法的原因
实施氧气处方政策
氧疗的管理和监测
卫生专业人员的教育
如何有效地处方氧气
开始氧疗
监测氧疗
脉搏血氧仪
动脉或动脉化毛细血管血气
生理监测:“跟踪和触发”系统
在氧疗的第一个小时内进行监测
随后的监测
何时增加氧疗
何时降低氧疗
医院处方图表氧气部分的工作实例
第12节断奶和停止氧疗
如何停止稳定患者的氧疗
第13节成果和审计
审计
审核遵守指南的情况
第14节指南的传播和实施
传播
当地准则
当地的氧气政策
氧气处方图表
员工教育
本地冠军
全国范围内实施的好处
第15节需要进一步研究的领域
附件1准则小组成员
每个成员对完整指南中章节的贡献清单
参考
指数
在线附录 - 可从http://www.brit-thoracic.org.uk获取
搜索策略
证据表
医院使用指南摘要
当地氧气政策的例子
救护车,社区和院前环境中紧急使用氧气的指南和流程图摘要
患者信息表
为医生提供紧急氧气使用讲座 - 可在以后获得
为护士,助产士,药剂师,物理治疗师和其他使用氧气的从业者提供紧急氧气使用教具
医院管理者和氧气冠军的关键点
初级保健管理人员,临床委托小组的要点
该指南的传播和实施
氧气是治疗低氧血症,而不是呼吸困难。尚未证实氧气对非低氧血症患者的呼吸困难感有任何一致的影响。
该指南的本质可以简单地概括为根据目标饱和范围规定氧气的要求,以及用于监测患者并保持在目标饱和范围内的氧气治疗者。
该指南建议,除了有高碳酸血症呼吸衰竭风险的患者或接受终末姑息治疗的患者外,所有急性病患者的氧饱和度均达到正常或接近正常水平。
临床医生必须记住,补充氧气可以改善氧合作用,但它不能治疗低氧血症的根本原因,必须作为紧急事项对其进行诊断和治疗。
在所有呼吸困难和急性病患者中,应通过脉搏血氧饱和度检查氧饱和度,“第五个生命体征”(必要时补充血气),并应在血氧测定结果的观察图上记录吸入氧浓度。(其他生命体征是脉率,血压,体温和呼吸频率)。
在使用紧急氧气的所有地方都必须提供脉搏血氧仪。如果饱和度下降≥3%或低于患者的目标范围,建议进行临床评估。
应使用公认的生理跟踪和触发系统(如国家预警评分)评估和监测重症监护区以外的所有重症患者(如重症监护病房(ICU),高依赖性单位(HDU),呼吸型HDU)。 (新闻)。
图1 - 医院急性低氧血症患者的氧气处方。任何FIO 2的增加必须在1小时内重复血气(或者如果意识水平恶化则更快)。*如果pH值<7.35([H +]> 45 nmol / L)且PaCO2正常或低,请调查并治疗代谢性酸中毒,并将SpO 2保持在94-98%。ABG,动脉血气; COPD,慢性阻塞性肺病; FiO 2,吸入氧气的分数; ICU,重症监护病房; NIV,无创通气; PaCO 2,动脉二氧化碳张力; PCO 2,二氧化碳张力; PO 2,氧气张力; SpO 2,通过脉搏血氧仪测量的动脉血氧饱和度。
氧应该被规定为达到94-98%的目标饱和度对于大多数重病患者或88-92%或患者特定的目标范围为那些在呼吸衰竭的风险(表1 ⇓ ⇓ - 4)。
最佳做法是在入院时规定所有住院患者的目标范围,以便在出现低氧血症意外临床恶化的情况下开始适当的氧疗,并确保预警评分(EWS)的血氧测定部分可以得到适当的得分。
目标饱和度应在药物图表上书写(或环绕)或输入电子处方系统(图1中的指导(图1))。
如果患者是低氧血症,需要中等水平的补充氧气的严重疾病
| 第8.11节 | ||
| 除非另有说明,否则初始氧疗法是2-6L / min(优选)的鼻导管或5-10L / min的简单面罩。 对于没有高碳酸血症呼吸衰竭风险且饱和度低于85%的患者,应以15 L / min的储库面罩开始治疗,推荐的初始氧饱和度目标范围为94-98%。如果没有血氧测定法,请按上述方法给氧,直至获得血氧测定或血气结果。如果使用鼻导管或简单面罩无法维持所需的饱和范围(并确保患者由高级医务人员评估),则更换为储液面罩。如果这些患者存在共存的COPD或其他高碳酸血症呼吸衰竭的危险因素,目标是血气检测结果的饱和度为88-92%,如果PCO则调整为94-98%2是正常的(除非有既往需要NIV或IMV的高碳酸血症呼吸衰竭病史)并在30-60分钟后重新检查血气,见表4。 |
| 补充评论 | 建议 | |
|---|---|---|
| 急性低氧血症(原因尚未确诊) | 如果初始SpO 2低于85%,则水库面罩为15 L / min ,否则鼻插管或简单面罩 需要水库面罩治疗的患者需要由高级工作人员进行紧急临床评估。 | 建议D1-D3 |
| 急性哮喘肺炎肺癌 | 建议F1-F3 | |
| 肺纤维化或其他间质性肺病的恶化 | 如果初始SpO 2低于85%,则储液器面罩为15 L / min ,否则为鼻插管或简单面罩 | 建议F4 |
| 气胸 | 如果患者是低氧血症,需要吸入或引流。大多数气胸患者不是低氧血症,不需要氧疗。 如果进行观察,请以15 L / min的速度使用水库面罩。目标是100%饱和度。(如果不需要引流,氧气会加速气胸的清除。) | 建议F5-F6 |
| 胸腔积液 | 大多数胸腔积液患者不是低氧血症。如果是低氧血症,通过引流积液治疗以及给予氧疗。 | 建议F7 |
| 肺栓塞 | 大多数肺栓塞轻微的患者不是低氧血症,不需要氧疗。 | 建议F8 |
| 急性心力衰竭 | 在肺水肿的情况下考虑CPAP或NIV。 | 建议F9-F10 |
| 严重贫血 | 主要问题是纠正贫血。大多数贫血患者不需要氧疗。 | 建议F11-12 |
| Postoperative breathlessness | Management depends on underlying cause. | Recommendation J1 |
COPD,慢性阻塞性肺病; CPAP,持续气道正压; IMV,有创机械通气; NIV,无创通气; PCO 2,动脉或动脉化二氧化碳张力; SpO 2,通过脉搏血氧仪测量的动脉血氧饱和度。
应密切监测患者的条件,但除非患者是低氧血症,否则不需要氧疗
| 第8.13节 | ||
| 如果是低氧血症,最初的氧疗法是2-6 L / min的鼻导管或5-10 L / min的简单面罩,除非饱和度低于85%(使用储液器面罩)或有高碳酸血症风险(见下文)。 除非另有说明,否则建议的初始目标饱和范围为94-98%。 如果没有血氧测定法,请按上述方法给氧,直至获得血氧测定或血气结果。 如果患者患有COPD或其他高碳酸血症呼吸衰竭的危险因素,目标是血气检测结果达到88-92%,但如果PCO 2正常则调整为94-98%(除非有呼吸衰竭病史需要NIV或IMV)并在30-60分钟后重新检查血气,见表4。 |
| 补充评论 | 建议 | |
|---|---|---|
| 心肌梗塞和急性冠状动脉综合征 | 大多数急性冠状动脉综合征患者不是低氧血症,在这种情况下,氧疗的益处和危害是未知的。不必要地使用高浓度氧气可能会增加梗塞面积。 | 建议F13 |
| 行程 | 大多数中风患者不是低氧血症。对于轻度中度中风的非低氧血症患者,氧疗可能有害。 | 建议F14 |
| 过度通气或呼吸功能障碍 | 排除器质性疾病。由焦虑或恐慌发作引起的纯过度通气的患者不太可能需要氧疗。 从纸袋中再吸入可能会导致低氧血症,不建议使用。 | 见8.13.3节 |
| 大多数中毒和药物过量(见表1中的一氧化碳中毒) | 低氧血症更可能是呼吸抑制药物,如果有的话可以给予解毒剂,例如纳洛酮用于阿片类药物中毒。 如果服用了呼吸抑制药物,检查血气以排除高碳酸血症。在酸吸入的情况下避免高血氧水平,因为有理论证据表明氧气在这种情况下可能是有害的。 监测2级或3级环境中的所有可能严重的中毒事件(高依赖性单位或重症监护病房)。 | 建议F15 |
| 中毒与百草枯或博来霉素 | 百草枯中毒或博来霉素肺损伤的患者可能会受到补充氧气的伤害。 除非患者是低氧血症,否则应避免吸氧。 目标饱和度为85-88%。 | 建议F16 |
| 代谢和肾脏疾病 | 大多数人不需要氧气(tachypnoea可能是由于这些患者的酸中毒) | 建议F17 |
| 急性和亚急性神经和肌肉状况导致肌肉无力 | 这些患者可能需要通气支持,他们需要仔细监测,包括肺活量测定。如果患者的氧气水平低于目标饱和度,则需要进行紧急血气测量,并且可能需要通气支持。 | 建议G4 |
| 怀孕和产科紧急情况 | 如果母亲不是低氧血症,氧疗可能对胎儿有害。 | 建议H1-H4 |
C OPD,慢性阻塞性肺病; IMV,有创机械通气; NIV,无创通气; PCO 2,动脉或动脉化二氧化碳张力。
COPD和其他需要控制或低剂量氧疗的病症
| 第8.12节 | ||
| 在血气可用之前,使用24%文丘里面罩,2-3 L / min或28%Venturi面罩,4 L / min或鼻导管,1-2 L / min,目标是氧饱和度为88-92有高碳酸血症危险因素但无既往呼吸性酸中毒史的患者%。如果PCO 2正常,则将目标范围调整为94-98%(除非有先前的NIV或IMV的历史)并在30-60分钟后重新检查血气。 |
| 补充评论 | 建议 | |
|---|---|---|
| COPD和其他引起固定气流阻塞的病症(如支气管扩张) | 如果酸中毒或可能对氧疗非常敏感,可能需要较低的范围。理想情况下使用“警报卡”来根据以前的血气结果指导治疗。如果呼吸频率高于30次呼吸/分钟,可将文丘里面罩流量增加50%。 | 建议G1-G2和第8.12.1节 |
| CF的恶化 | 如果可能,如果不与区域中心讨论或根据与区域CF中心商定的协议进行管理,则尽可能接纳区域CF中心。理想情况下使用“警示卡”来指导治疗。如果呼吸频率高于30次呼吸/分钟,可将文丘里面罩流量增加50%。 | 建议G1,G3,G6 |
| 神经肌肉疾病,神经系统疾病和胸壁畸形 | 可能需要通气支持。 | 建议G1,G4,G6 |
| 高碳酸血症呼吸衰竭的风险 | ||
| 病态肥胖 | 建议G1,G5,G6 |
CF,囊性纤维化; COPD,慢性阻塞性肺病; IMV,有创机械通气; NIV,无创通气; PCO 2,动脉或动脉化二氧化碳张力。
氧气应由接受氧气管理培训的工作人员进行。
这些人员应使用适当的设备和流量以达到目标饱和范围(图2(图2))。
工作人员应接受使用各种不同氧气输送装置的培训,以确保安全输送氧气。
图2 - 医院普通病房的氧气管理流程图。*对于文丘里口罩,如果呼吸率> 30,则需要更高的流速。ABG,动脉血气; COPD,慢性阻塞性肺病; EPR,电子病历; EWS,预警评分; 新闻,国家预警分数; SpO 2,通过脉搏血氧仪测量的动脉血氧饱和度。
CaO 2的调节。肺泡毛细血管单位。CaO 2,血氧含量; PaCO 2,动脉二氧化碳和氧气张力; PaO 2,动脉血氧分压; PACO 2,肺泡二氧化碳张力; PAO 2,肺泡氧张力; PICO 2,激发二氧化碳张力; PIO 2,激发氧气张力; PVCO 2,静脉二氧化碳张力; PVO 2,静脉氧张力。
应在患者监测表上记录氧饱和度和输送系统(包括流速)。
应调节氧气输送装置和流速,以使氧饱和度保持在目标范围内。如果由于饱和度下降需要开始或增加氧疗,则需要及时进行临床评估。
应规定氧气并在每轮药物的药物图表上输入签名。
在具有令人满意的氧饱和度的稳定患者中应减少氧气。
一旦患者能够在呼吸空气的目标范围内或之上保持饱和,就应该停止使用氧气,但是如果将来恶化,应该保留目标范围的处方并指导EWS / NEWS。
A1:本指南建议除了有高碳酸血症呼吸衰竭风险的患者(D级)外,所有急性病患者的氧饱和度均达到正常或接近正常水平。
A2:没有高碳酸血症呼吸衰竭风险的急性病患者的推荐目标饱和度范围是94-98%(D级)。
A3:对于已知慢性阻塞性肺病(COPD)或其他已知的高碳酸血症性呼吸衰竭危险因素(如病态肥胖,囊性纤维化(CF),胸壁畸形或神经肌肉疾病或与支气管扩张相关的固定气流阻塞)的大多数患者,在血气结果可用之前,建议目标饱和度范围为88-92%(COPD为A级,其他条件为D级)。
A4:大多数非低氧血症无呼吸患者不会从氧疗中受益,但患者在目标饱和度范围内的氧饱和度突然降低≥3%应该能够更快地评估患者(和血氧计信号),因为这可能是急性疾病的第一个证据(D级)。
A5:由于仰卧位的氧合作用减少,理想情况下应该让完全清醒的低氧血症患者保持最直立的姿势(或患者最舒适的姿势),除非有充分理由使患者固定(例如,骨骼或脊髓损伤)(D级)。
B1:训练有素的临床医生应通过测量呼吸频率,脉搏率,血压和体温以及评估循环血容量和贫血来评估所有急性病患者(见第7节)。如果患者被认为患有严重危及生命的疾病,应尽早寻求重症监护专家或其他学科的专家协助,临床医生应准备在必要时呼吁提供帮助,包括在院前护理中呼叫999救护车或致电复苏团队或ICU外展团队进行医院护理(D级)。
B2:氧饱和度,“第五个生命体征”,应由经过培训的工作人员使用脉搏血氧仪检查所有呼吸困难和急性病患者(必要时补充血气),并在观察时记录吸入氧气装置和流速血氧测定结果图表(D级)。
B3:急性不适患者的初步临床评估和随后的监测应包括使用公认的生理“追踪和触发”系统,例如可能由于低氧血症引起的临床检查,需要补充氧气或其他原因的新闻(等级) d)。
B4:对于有高碳酸血症呼吸衰竭风险的患者,建议使用2017年新闻图表的相关部分。如果氧饱和度低于或高于目标范围(D级),则授予积分。
对疑似低氧血症患者进行临床评估的良好实践点
应尽可能在急性呼吸困难的患者中进行病史,并且可能指出特定急性疾病的诊断,例如肺炎或肺栓塞或慢性病如COPD,哮喘或心力衰竭的恶化。
永远不要停止氧疗,以便在明显需要氧疗的患者的室内空气中进行血氧测量。
应紧急进行体格检查。这可能提供特定诊断的证据,例如心力衰竭或大量胸腔积液,但是直到胸部X光片等检查结果可用之前,仍然未确诊呼吸困难的原因。
通过脉搏血氧仪(SpO 2)测量记录的动脉血氧饱和度,并考虑不明原因混淆和激动的患者的血气评估,因为这可能是低氧血症和/或高碳酸血症的特征(紫绀是一种难以自信地记录的体征,特别是在贫困中轻或患有贫血或多尿症的病人)。
仔细测量呼吸频率和心率,因为在低氧血症患者中,痉挛和心动过速比紫绀的身体发现更常见。
应对任何“跟踪和触发”系统进行适当的更改,以便在有高碳酸血症呼吸衰竭风险的患者中实现较低的目标范围。如果在目标范围内,这些患者的饱和度应该没有EWS点,如果氧饱和度低于目标范围,或者在呼吸氧气时饱和度超过目标范围,则应该得分。2017年更新的NEWS图表有一个特殊的血氧测量测量部分,用于目标范围为88-92%的患者,建议所有医院都应使用2017年新闻图表(见建议B4)。
正常SpO 2的存在并不否定对血气测量的需要,特别是如果患者正在进行补充氧疗。在具有正常氧张力(PO 2)但血液pH值或二氧化碳张力异常(PCO 2)或由于贫血引起的低血氧含量的患者中,脉搏血氧测定法将是正常的。出于这个原因,在这些测量可能影响患者结果的所有情况下,需要尽早进行血气和全血细胞计数测试。
所有使用血氧计的临床工作人员必须接受使用培训,并了解血氧测定的局限性。(血氧测定法是一种有价值的临床工具,但受人工制品和解释错误的影响)。
C1:对于重症患者或有休克或低血压(收缩压<90 mm Hg)的患者,应从动脉样本中获取初始血气测量值(见7.1.3和8.4和8.5节)。对于需要血气采样的大多数患者,可以使用动脉血气(ABG)或动脉化的耳垂血气来获得pH和PCO 2的精确测量。然而,PO 2在耳垂血气样本中的准确度较低(它低估了PO 2 0.5-1 kPa),因此如果使用耳垂血气标本,应仔细监测血氧饱和度,如果有的话,应采取重复动脉标本关注毛细管样品的准确性(D级)。
C2: Local anaesthesia should be used for all ABG specimens except in emergencies (grade A).
C3: Blood gases should be checked in the following situations:
All critically ill patients (grade D).
Unexpected or inappropriate fall in SpO2 below 94% in patients breathing air or oxygen or any patient requiring oxygen to achieve the above target range. (Allowance should be made for transient dips in saturation to 90% or less in normal participants during sleep) (grade D).
Deteriorating oxygen saturation (fall of ≥3%) or increasing breathlessness in a patient with previously stable chronic hypoxaemia (eg, severe COPD) (grade D).
Most previously stable patients who deteriorate clinically and require increased fraction of inspired oxygen (FiO2) to maintain a constant oxygen saturation (grade D).
Any patient with risk factors for hypercapnic respiratory failure who develops acute breathlessness, deteriorating oxygen saturation, drowsiness or other features of carbon dioxide retention (grade D).
Patients with breathlessness who are thought to be at risk of metabolic conditions such as diabetic ketoacidosis or metabolic acidosis due to renal failure (grade D).
Any other evidence from the patient's medical condition that would indicate that blood gas results would be useful in the patient's management (eg, an unexpected change in ‘track and trigger’ systems such as a sudden rise of several units in the NEWS or an unexpected fall in oxygen saturation of 3% or more, even if within the target range) (grade D).
Good practice point: patients requiring increased concentration of oxygen
The requirement for an increased concentration of oxygen is an indication for urgent clinical reassessment of the patient (and repeat blood gas measurements in most instances, see recommendations W13 and W18 for exceptions).
Initial oxygen therapy in critical illness is covered in the next section.
D1: For acutely breathless patients not at risk of hypercapnic respiratory failure who have saturations below 85%, treatment should be started with a reservoir mask at 15 L/min in the first instance (see figures 1–2 (charts 1–2) and table 2 and sections 8.9 and 10).* The oxygen concentration can be adjusted downwards (using nasal cannulae at 1–6 L/min or a simple face mask at 5–10 L/min) to maintain a target saturation of 94–98% once the patient has stabilised (grade D).
D2: In other cases of acute hypoxaemia without critical illness or risk factors for hypercapnic respiratory failure, treatment should be started with nasal cannulae (or a simple face mask if cannulae are not tolerated or not effective) with the flow rate adjusted to achieve a saturation of 94–98% (grade D).
D3: If medium-concentration therapy with nasal cannulae or a simple face mask does not achieve the desired saturation, change to a reservoir mask and seek senior or specialist advice (grade D).
Good practice point
High-flow nasal oxygen using specialised equipment should be considered as an alternative to reservoir mask treatment in patients with acute respiratory failure without hypercapnia.
*For initial management of patients at risk of hypercapnic respiratory failure, see recommendations G1 and G2.
E1: Use the highest feasible inspired oxygen for ventilation during cardiopulmonary resuscitation (CPR; see table 1 and section 8.10). Once spontaneous circulation has returned and arterial blood oxygen saturation can be monitored reliably, aim for a target saturation range of 94–98% and take an ABG sample to guide ongoing oxygen therapy. If the blood gas shows hypercapnic respiratory failure, reset the target range to 88–92% or consider mechanical ventilation (grade D).
E2: In critical illness, including major trauma, sepsis, shock and anaphylaxis, initiate treatment with a reservoir mask at 15 L/min and aim at a saturation range of 94–98%. This advice also applies to patients with critical illness who have risk factors for hypercapnia pending the results of blood gas measurements and expert assessment. In patients with spontaneous circulation and a reliable oximetry reading it may be possible to maintain a saturation of 94–98% using lower concentrations of oxygen (grade D)
E3: In cases of drowning, aim at an oxygen saturation of 94–98% once spontaneous circulation is restored (grade D).
E4: In patients with acute seizures due to epilepsy or other causes, high-concentration oxygen should be administered until a satisfactory oximetry measurement can be obtained and clinicians should then aim for an oxygen saturation of 94–98% or 88–92% if the patient is at risk of hypercapnic respiratory failure (grade D).
E5: In cases of major head injury, aim at an oxygen saturation of 94–98%. Initial treatment should involve high-concentration oxygen from a reservoir mask at 15 L/min pending availability of satisfactory blood gas measurements or until the airway is secured by intubation (grade D).
E6: In cases of carbon monoxide poisoning, an apparently ‘normal’ oximetry reading may be produced by carboxyhaemoglobin, so aim at an oxygen saturation of 100% and use a reservoir mask at 15 L/min irrespective of the oximeter reading and arterial oxygen tension (PaO2) (grade D).
Respiratory conditions with low risk of hypercapnic respiratory failure
F1: In acute asthma, aim at an oxygen saturation of 94–98% (see tables 2 and 3 and sections 8.11 and 8.13) (grade D).
F2: In cases of pneumonia who are not at risk of hypercapnic respiratory failure, aim at an oxygen saturation of 94–98% (grade D).
F3: In acute breathlessness due to lung cancer, aim at an oxygen saturation of 94–98% unless there is coexisting COPD. See also ‘Oxygen use in palliative care’ section 8.17 (grade D).
F4: In acute deterioration of pulmonary fibrosis or other interstitial lung diseases, aim at an oxygen saturation of 94–98% or the highest possible if these targets cannot be achieved (grade D).
F5: In most cases of pneumothorax, aim at an oxygen saturation of 94–98% if the patient is not at risk of hypercapnic respiratory failure (grade D).
F6:对于无引流的医院观察的气胸患者,建议使用高浓度氧气(通过储液面罩的流速为15 L / min),除非患者有高碳酸血症呼吸衰竭的风险(D级)。
F7:在胸腔积液中,目标是氧饱和度为94-98%(如果患者存在高碳酸血症呼吸衰竭的风险,则为88-92%)(D级)。
F8:在肺栓塞中,目标是氧饱和度为94-98%(如果患者有高碳酸血症呼吸衰竭的风险,则为88-92%)(D级)。
非呼吸系统疾病
F9:在急性心力衰竭时,目标是氧饱和度为94-98%(如果患者存在高碳酸血症呼吸衰竭的风险,则为88-92%)(D级)。
F10:持续气道正压通气(CPAP)与夹带氧气或高流量加湿鼻腔氧气维持饱和度94-98%(如果有高碳酸血症风险,则为88-92%)应被视为改善气体交换的辅助治疗方法。心源性肺水肿患者对标准治疗没有反应(如果存在共存的高碳酸血症和酸中毒,则为无创通气(NIV))(B级)。
F11:在贫血症中,如果患者处于高碳酸血症呼吸衰竭的风险(D级),则氧饱和度为94-98%或88-92%。
好的做法点
通过输血纠正贫血应该基于国家指南。
F12:在镰状细胞危象和急性胸部综合征中,目标是氧饱和度为94-98%或者针对个体患者通常的饱和水平(D级)。
关于镰状细胞危象的良好实践点
如果对镰状细胞危象期间血氧测定的可靠性有任何疑问,应采集动脉或动脉化毛细血管血气。
F13:在心肌梗塞和急性冠状动脉综合征中,如果患者处于高碳酸血症呼吸衰竭的风险(D级),则氧饱和度为94-98%或88-92%。
F14:中风患者应避免高浓度氧气,除非需要维持正常的氧饱和度。如果患者处于高碳酸血症呼吸衰竭的风险(D级),目标是氧饱和度为94-98%或88-92%。
关于中风管理的良好实践要点
在急性卒中患者和所有低氧血症治疗患者中,应至少每4小时监测一次氧饱和度。
卒中后低氧血症患者需要进行医学检查以确定并治疗病因。
只有在气道被清除后才能给氧气,并且如果患者有高碳酸血症呼吸衰竭的风险,则应达到氧饱和度达到94-98%或88-92%所需的最低浓度。
Oxygen should be given via nasal cannulae, unless there are clear indications for a different oxygen delivery system.
Patients with stroke and cardiorespiratory comorbidities should be positioned as upright as possible, in a chair if possible (see recommendation A5).
Patients with a reduced level of consciousness after stroke should be nursed in the recovery position with the paralysed side lowest.
Good practice points regarding patients with suspected hyperventilation
Organic illness must be excluded before making a diagnosis of hyperventilation.
Patients with a definite diagnosis of hyperventilation should have their oxygen saturation monitored. Those with normal or high SpO2 do not require oxygen therapy.
Rebreathing from a paper bag can be dangerous and is NOT advised as a treatment for hyperventilation.
F15: In most poisonings, aim at an oxygen saturation of 94–98% unless the patient is at risk of hypercapnic respiratory failure (grade D).
F16: In poisoning by paraquat and poisoning by bleomycin, give oxygen only if the saturation falls below 85% and reduce or stop oxygen therapy if the saturation rises above 88% (grade D).
F17: In most metabolic and renal disorders, aim at an oxygen saturation of 94–98% unless the patient is at risk of hypercapnic respiratory failure (grade D).
F18: For patients with cluster headaches, oxygen should be administered using a flow of at least 12 L/min from a reservoir mask and home oxygen should be provided (grade D).
G1 (also A3): For most patients with known COPD or other known risk factors for hypercapnic respiratory failure (eg, morbid obesity, CF, chest wall deformities or neuromuscular disorders or fixed airflow obstruction associated with bronchiectasis), a target saturation range of 88–92% is suggested pending the availability of blood gas results (grade A for COPD, grade D for other conditions).
G2: Some patients with COPD and other conditions are vulnerable to repeated episodes of hypercapnic respiratory failure. In these cases it is recommended that treatment should be based on the results of previous blood gas estimations during acute exacerbations. For patients with prior hypercapnic failure (requiring NIV or intermittent positive pressure ventilation) who do not have an alert card, it is recommended that low-concentration oxygen treatment should be started using a 24% Venturi mask at 2–3 L/min (or a 28% Venturi mask at 4 L/min or nasal cannulae at 1–2 L/min if a 24% mask is not available) with an initial target saturation of 88–92% pending urgent blood gas results. These patients should be treated as a high priority by emergency services and the oxygen concentration should be reduced if the saturation exceeds 92% but increased if it falls below 88% (grade D).
Good practice points for COPD and other conditions that may cause hypercapnic respiratory failure
Diagnosis of COPD or suspected exacerbation of COPD
If the diagnosis is unknown, patients over 50 years of age who are long-term smokers with a history of chronic breathlessness on minor exertion such as walking on level ground and no other known cause of breathlessness should be treated as having suspected COPD for the purposes of this guideline.
Spirometry should be measured at least once during hospital admissions for suspected COPD (as per National Institute of Health and Care Excellence (NICE) COPD guideline1). Measurement of spirometry may confirm (or exclude) a diagnosis of airflow obstruction and the forced expiratory volume in 1 s (FEV1) level is a useful indicator of disease severity in COPD.
Immediate management of patients with known or suspected COPD
If the saturation remains below 88% in prehospital care despite a 28% Venturi mask, change to nasal cannulae at 2–6 L/min or a simple face mask at 5 L/min with target saturation of 88–92% and alert the accident and emergency (A&E) department that the patient is to be treated as a high priority.
Patients with a respiratory rate >30 breaths/min should have the flow rate from Venturi masks set above the minimum flow rate specified for the Venturi mask packaging to compensate for the patient's increased inspiratory flow (see figure 11B). Increasing the oxygen flow rate into a Venturi mask does not increase the concentration of oxygen which is delivered.
Patients with a significant likelihood of severe COPD or other illness that may cause hypercapnic respiratory failure should be triaged as very urgent on arrival in hospital emergency departments and blood gases should be measured on arrival in hospital.
Prior to availability of blood gas measurements, use a 24% Venturi mask at 2–3 L/min or nasal cannulae at 1–2 L/min or 28% Venturi mask at 4 L/min and aim for an oxygen saturation of 88–92%.
Initial hospital management of patients with exacerbation of COPD
Patients with exacerbations of COPD need careful monitoring for hypercapnic respiratory failure with respiratory acidosis which may develop in the course of a hospital admission even if the initial blood gases were satisfactory.
Avoid excessive oxygen use in patients with COPD. The risk of respiratory acidosis in patients with hypercapnic respiratory failure is increased if the PaO2 is above 10.0 kPa due to previous excessive oxygen use.
If following blood gas measurements the pH and PCO2 are normal, aim for an oxygen saturation of 94–98% unless there is a history of previous hypercapnic respiratory failure requiring NIV or intermittent positive pressure ventilation or if the patient's usual oxygen saturation when clinically stable is below 94% (these patients should have a target range of 88–92%). Blood gases should be repeated at 30–60 min to check for rising PCO2 or falling pH.
Recheck blood gases after 30–60 min (or if there is evidence of clinical deterioration) for all patients with COPD or other risk factors for hypercapnic respiratory failure even if the initial PCO2 measurement was normal.
如果PCO 2升高但pH值≥7.35(H + ] ≤45nmol / L)和/或高碳酸氢盐水平(> 28 mmol / L),则患者可能患有长期高碳酸血症; 维持这些患者的目标范围为88-92%。应在30-60分钟内重复血气检查以检查PCO 2升高或pH值下降。
如果患者是高碳酸血症(PCO 2 > 6 kPa或45 mm Hg)和酸中毒(pH <7.35或[H + ]> 45 nmol / L),如果呼吸性酸中毒持续超过30分钟,则开始用靶向氧疗法进行NIV治疗启动标准医疗管理。
对于使用文丘里面罩的患者,一旦患者稳定,可考虑从文丘里面罩换成鼻插管。
对于使用长期家庭氧气(LTOT)治疗严重COPD的患者,如果88-92%的标准范围需要对患者通常的氧疗进行不适当的调整,则高级临床医生应考虑设定患者特异性目标范围。在医院。
(A)(a)文丘里口罩,(b)可用浓度范围,(c)文丘里阀的操作。对于24%文丘里掩模,典型的2L / min的氧气流量使总气体流量为51L / min。对于28%文丘里掩模,4L / min氧气流量使总气体流量为44L / min(表13)。(B)文丘里面罩的建议流速和高呼吸率的调整。RM,水库面具; RR,相对风险。
Oxygen saturation response to treatment with 24%, 28% and 35% oxygen in hypoxaemic patients with COPD. This illustration shows actual oxygen saturations from Warrel et al85 and King et al293 together with calculated saturations from DeGaute et al,461 Schiff and Massaro292 and Bone et al462 (two different groups of patients). COPD, chronic obstructive pulmonary disease.
Good practice points
Management of hypercapnia or respiratory acidosis due to excessive oxygen therapy (avoidance of life-threatening rebound hypoxaemia)
If a patient is suspected to have hypercapnic respiratory failure due to excessive oxygen therapy, the oxygen therapy must be stepped down to the lowest level required to maintain a saturation range of 88–92%. This may be achieved using 28% or 24% oxygen from a Venturi mask or 1–2 L/min via nasal cannulae depending on oxygen saturation and subsequent blood gas measurements.
Sudden cessation of supplementary oxygen therapy can cause life-threatening rebound hypoxaemia with a rapid fall in oxygen saturations below the starting oxygen saturation prior to the start of supplementary oxygen therapy.
G3: Initial oxygen treatment of CF exacerbations should be similar to the initial oxygen treatment of COPD exacerbations with target saturation 88–92% (see sections 8.12.1–8.12.2; grade D).
G4: In the initial management of musculoskeletal and neurological disorders with acute respiratory failure or acute-on-chronic respiratory failure, aim at an oxygen saturation of 88–92% and measure blood gases to determine if NIV will be required (grade D).
Good practice point regarding patients with neurological disorders
✓ Patients with respiratory failure due to neurological disorders or muscle disease are at high risk of dying and require urgent assessment to determine if they are likely to require non-invasive or invasive ventilator support rather than oxygen therapy. Monitor these patients with blood gases and regular spirometry (forced vital capacity). Patient's wishes regarding this form of treatment should be established as early as possible in the course of the illness, ideally before an acute episode has developed.
G5: Morbidly obese patients (body mass index (BMI)>40 kg/m2), even without evidence of coexistent obstructive sleep apnoea (OSA) are at risk of hypoventilation and should be given titrated oxygen to maintain a target saturation of 88–92% (grade D).
G6: NIV should be considered for hypercapnic patients with COPD, CF, neuromuscular disorders or morbid obesity who are at risk of hypercapnic respiratory failure if the pH is <7.35 or [H+]>45 nmol/L (grade D). See BTS/ICS Guideline for the ventilatory management of acute hypercapnic respiratory failure (ref 299).
H1: Women who suffer from major trauma, sepsis or acute illness during pregnancy should receive the same oxygen therapy as any other seriously ill patients, with a target oxygen saturation of 94–98%. The same target range should be applied to women with hypoxaemia due to acute complications of pregnancy (eg, collapse related to amniotic fluid embolus, eclampsia or antepartum or postpartum haemorrhage) (grade D).
H2: Women with underlying hypoxaemic conditions (eg, heart failure) should be given supplemental oxygen during labour to achieve an oxygen saturation of 94–98% unless they are at risk of hypercapnic respiratory failure (target range 88–92%) (grade D).
H3: Pregnant women who are fully conscious with no cardiovascular compromise may be managed in the sitting position or if lying down should use the full left lateral position (grade D).
H4: Pregnant women above 20 weeks gestation (uterine fundus at or above the level of the umbilicus) who are at risk of developing associated cardiovascular compromise (eg, trauma, vaginal bleeding, etc) should be positioned to avoid aortocaval compression by using left lateral tilt, manual uterine displacement or by placing them in a full left lateral position (grade D).
H5: Women who are more than 20 weeks pregnant with evidence of hypoxaemia associated with reduced consciousness or those requiring respiratory or cardiovascular support or CPR should be managed with left lateral tilt or manual uterine displacement (ideally to the left) to improve cardiac output and oxygen delivery (grade D).
H6: The use of oxygen supplementation during intrauterine fetal resuscitation during labour was widespread in the past but there is no evidence of benefit. There is weak evidence of harm to the fetus if supplemental oxygen is given for long periods during uncomplicated labour. Overall, the use of oxygen during labour is only required when there is evidence of maternal hypoxaemia (oxygen saturation <94%) (grade D).
J1:在围手术期和术后期间不建议常规使用高氧血症,以减少术后恶心和呕吐的发生率(D级)。
J2:所有涉及清醒镇静的程序都需要在手术前和手术过程中以及恢复期间通过脉搏血氧仪连续监测氧饱和度,尤其是纤维支气管镜检查和上消化道(GI)内镜检查,其中动脉血氧饱和度降低(SaO)2)是常见的,特别是同时使用镇静剂(C级)。
J3:显着的动脉氧饱和度下降(SpO 2 <90%或下降4%或更长时间延长(内镜检查过程中> 1 min))应通过补充氧气进行校正,目的是达到94-98%的目标氧饱和度,或有高碳酸血症呼吸衰竭风险者(D级)的88-92%。
J4:心肺综合征患者的复杂上消化道内镜检查或手术尤其可能导致低氧血症,并且还可能导致高碳酸血症,特别是如果患者严重镇静。如果此类患者需要长期给予氧气,建议测量血气。不建议常规给予氧气,因为它可能会延迟对呼吸衰竭的识别(D级)。
J5:在清醒镇静程序的所有阶段,对患者进行持续的临床评估至关重要,监测二氧化碳图或经皮二氧化碳水平可能是识别早期呼吸抑制的有用辅助手段(D级)。
J6:在需要清醒镇静的手术后的恢复期间,应滴定补充氧气,使大多数患者的目标饱和度达到94-98%,高碳酸血症呼吸衰竭风险者达到88-92%(见10.5.1) d)。
在围手术期护理中与氧气使用相关的良好实践要点
对于大多数手术患者,建议目标饱和度为94-98%,除了那些有高碳酸血症呼吸衰竭风险的患者,应达到88-92%的范围。
尽管随机研究缺乏证据,但建议对术后患者进行脉搏血氧饱和度监测。
使用患者自控镇痛(PCA)的患者应该进行两小时的血氧测定观察,因为存在低氧血症的风险。应施用氧气以使患者保持在适当的目标饱和范围内。
大多数患有PCA的患者建议目标饱和度为94-98%,除了那些有高碳酸血症呼吸衰竭风险的患者,应达到88-92%的范围。
关于围手术期高氧血症的潜在益处和风险的平衡存在相互矛盾的证据,以降低选择性手术中手术部位感染的风险,并且在具有紧急外科手术的患者中没有证据表明这种做法。特定程序需要更多的试验,并且需要有关癌症患者长期死亡风险的更多信息。与此同时,在临床试验之外,不应将氧气用于此适应症。
K1:姑息治疗患者的氧气使用应限于SpO 2持续<90%的患者或报告显着缓解氧气呼吸困难的患者。在非低氧血症患者中,应在氧气之前尝试阿片类药物和非药物治疗措施(B级)。
K2:一般而言,在生命的最后几天,在以舒适为重点的护理中监测氧饱和度或PaO 2没有任何作用。如果患者看起来舒服,氧气水平是无关紧要的,不应影响护理(D级)。
姑息治疗中与氧气使用相关的良好实践要点
用于姑息治疗患者呼吸困难的症状缓解的氧疗比简单的低氧血症校正更复杂。请考虑以下问题:
Consider early involvement of palliative care specialists and physiotherapists;
As breathlessness is a multifactorial sensation—a comprehensive assessment of contributing factors (such as anxiety) should be carried out.
Low-dose opioids should be considered because they are effective for the relief of breathlessness in palliative care patients.
A trial of a hand held fan to help relieve breathlessness is recommended prior to trial of oxygen.
Oxygen use has to be tailored to the individual and a formal assessment made of its efficacy for reducing breathlessness and improving quality of life for that person.
Oxygen therapy should not be continued in the absence of patient benefit or where its disadvantages (eg, discomfort of masks or nasal cannulae, drying of mucous membranes) outweigh any likely symptomatic benefit.
Use of helium–oxygen mixtures (Heliox) see section 8.18
L1: There is insufficient evidence to support the use of Heliox either as an inhaled gas or as the driving gas for nebuliser therapy in adult patients with acute exacerbations of asthma or acute exacerbations of COPD (AECOPD) except as part of randomised clinical trials or in exceptional circumstances (grade D).
L2: A therapeutic trial of Heliox is reasonable in patients with mechanical upper airway obstruction or postoperative stridor (grade D).
L3: Heliox use for patients with asthma or COPD should be considered only in clinical trials or in specialist hands for severe exacerbations that are not responding to standard treatment (and in patients with COPD where there are contraindications to intubation) (grade D)
M1: The use of Entonox gas mixture for analgesia should be avoided if possible in patients at risk of hypercapnic respiratory failure (grade D).
Use of CPAP in the perioperative period and for pulmonary oedema (see section 8.19)
N1: Patients with diagnosed sleep-disordered breathing established on CPAP undergoing surgery should bring their machines with them and use them in the preoperative and postoperative period. If adequate saturations are not achieved despite CPAP therapy then assess for worsening ventilation with blood gases and oxygen should be entrained to achieve a saturation of 88–92% (grade D).
N2: CPAP with entrained oxygen to maintain saturation 94–98% should be considered as an adjunctive treatment to improve gas exchange in patients with cardiogenic pulmonary oedema who are not responding to standard treatment in hospital care or in prehospital care (grade B).
Good practice point, high-flow humidified nasal oxygen via nasal cannulae
High-flow humidified nasal oxygen should be considered as a potentially superior alternative to reservoir mask treatment in patients with acute respiratory failure without hypercapnia.
The prefix O is not in use for recommendations.
P1: When oxygen is required by patients with prior tracheostomy or laryngectomy, a tracheostomy mask (varying the flow as necessary) should achieve the desired oxygen saturation (tables 1⇑⇑–4). An alternative delivery device, usually a T-piece device fitted directly to the tracheostomy tube, may be necessary if the patient deteriorates (grade D).
Q1: Humidification is not required for the delivery of low-flow oxygen (mask or nasal cannulae) or for the short-term use of high-flow oxygen. It is not therefore required in prehospital care. Pending the results of clinical trials, it is reasonable to use humidified oxygen for patients who require high-flow oxygen systems for more than 24 hours or who report upper airway discomfort due to dryness (grade D).
Q2: In the emergency situation, humidified oxygen use can be confined to patients with tracheostomy or an artificial airway although these patients can be managed without humidification for short periods of time (eg, ambulance journeys) (grade D).
Q3: Humidification may also be of benefit to patients with viscous secretions causing difficulty with expectoration. This benefit can be achieved using nebulised normal saline (grade D).
Q4: Bubble bottles which allow a stream of oxygen to bubble through a container of water should not be used because there is no evidence of a clinically significant benefit but there is a risk of infection (grade D).
Good practice points related to humidified oxygen therapy
Consider use of a large volume oxygen humidifier device for patients requiring high-flow rates or longer term oxygen, especially if sputum retention is a clinical problem.
In the absence of an artificial airway the decision to humidify supplemental oxygen needs to be made on an individual basis but this practice is not evidence-based.
R1:对于哮喘患者,雾化器应由管道氧气或配有高流量调节器的氧气瓶驱动,该流量调节器能够提供> 6 L / min的流速。当雾化器治疗完成时,应将患者换回他/她通常的氧气面罩或套管。如果气瓶不产生这种流速,则应使用气动雾化器(带电动压缩机),鼻导管以2-6 L / min的速度补充氧气,以维持适当的氧饱和度(D级)。
R2:当对患有高碳酸血症的患者给予雾化支气管扩张剂时,应使用超声雾化器或由压缩空气驱动的喷射雾化器给予它们,如果需要,应通过鼻导管同时给予补充氧气以维持氧饱和度88-92%。对于在血气结果可用之前有高碳酸血症呼吸衰竭风险的患者,应采取相同的预防措施,并在治疗期间连续监测血氧饱和度。对于有高碳酸血症呼吸衰竭风险的患者完成雾化治疗后,应重新开始其先前的靶向氧疗(D级)。
好的练习点
给予雾化治疗时不要发生低氧血症:
对于低氧血症患者,在雾化治疗期间应继续进行氧疗。
在救护车中驾驶气体进行雾化治疗
在救护人员治疗期间,氧气驱动的雾化器应该用于哮喘患者,并且可以在没有气动压缩机系统的情况下用于患有COPD的患者。如果已知COPD患者使用氧气,其使用应限制在6分钟。这将提供大部分雾化药物剂量但限制高碳酸血症呼吸衰竭的风险(第10.4节)。鼓励救护车服务探索引入电池供电,气动喷雾器或便携式超声波雾化器的可行性。
S1:每个医疗保健机构都应该有一个标准的氧气处方文件,或者最好是所有药物处方卡上的指定氧气部分或电子处方系统中的氧气指导处方(D级)。
S2:应始终提供氧气处方,但必须立即开始并且回顾性记录(D级)的突发疾病除外。
S3:医生和其他开处方者应使用目标饱和度范围(第8,9和11节)开氧,并签署药物图表或电子处方令(D级)。
S4:应为所有住院患者规定氧饱和度范围。这将确保每个患者在需要时接受适当的氧疗。它还将确保所有临床医生都知道他们所照顾的每个患者的适当氧气目标范围(D级)。
与患者开处方和给予氧疗相关的良好实践要点
应使用目标饱和范围在药物图表或电子处方系统上规定氧气。
应将氧气规定为目标饱和范围,而不是规定固定浓度的氧气或FiO 2(参见建议A1,A2,A4和A5)
In most emergency situations, oxygen is given to patients immediately without a formal prescription. The lack of a prescription should never preclude oxygen being given when needed in an emergency situation. However, a subsequent written record must be made of what oxygen therapy has been given to every patient in a similar manner to the recording of all other emergency treatment.
If a patient has an oxygen alert card, initial oxygen therapy should be based on the guidance on the card until the results of blood gases are available.
T1: Pulse oximetry must be available in all locations where emergency oxygen is being used by healthcare professionals (see also the limitations of using pulse oximetry section 7.1.2) (grade D).
T2: All documents which record oximetry measurements or blood gas results should state whether the patient is breathing air or a specified oxygen delivery device and flow rate using the abbreviations shown in table 5 (grade D).
Abbreviations for oxygen devices for use on bedside charts
T3: In all situations where repeated blood gas measurements are required, they should be measured as soon as possible, usually within 30 min of any treatment change, to determine if the proposed target saturations are appropriate. Consider the use of an indwelling arterial catheter if multiple samples are likely to be required (grade D).
T4: Adjustments should only be made by registered staff who have been trained to administer oxygen. If the oxygen saturation falls below the prespecified range, the concentration of oxygen should be increased; if the saturation rises above this range, the oxygen concentration should be reduced. If the monitoring of oxygen saturation is performed by unregistered staff (eg, healthcare assistants), there must be a clear protocol in place which requires that they should inform staff who are trained to administer oxygen if the oxygen saturation is above or below the target saturation (grade D).
Good practice points related to administration of oxygen therapy
For hypoxaemic patients, oxygen therapy should continue during other treatments such as nebulised therapy. Clinicians should assess the clinical status of the patient prior to prescribing oxygen and the patient's condition should be reassessed frequently during oxygen use (see recommendations B1-B3).
The administering healthcare professional should note the oxygen saturation before starting oxygen therapy whenever possible but never discontinue or delay oxygen therapy for seriously ill patients (see recommendation B2).
The healthcare professional should start oxygen therapy using an appropriate delivery system and flow rate as specified in sections 8 –10 of this guideline. The target oxygen saturation should be documented on the respiratory section of the observation chart.
Whenever possible, patients should be given an oxygen information sheet (example in web appendix 6 of this guideline on the BTS website).
Staff should check the oxygen supply and connections on a regular basis because there have been serious incidents due to disconnection or misconnection of oxygen supplies.
Staff must ensure that adequate oxygen is provided during transfers and while patients are in diagnostic departments. Additionally, oxygen saturation should be monitored continuously for seriously ill patients who require escorted transfers. This is because there have been serious incidents involving accidental discontinuation of oxygen or cylinders running out during interward transfers or transfers to other departments such as for x-rays.
U1: Lower the oxygen concentration if the patient is clinically stable and the oxygen saturation is above the target range or if it has been in the upper zone of the target range for some time (usually 4–8 hours) (grade D).
U2: If the target saturation is maintained, the new delivery system and flow should be continued. Repeat blood gas measurements are not required. If the patient is stable the process can be repeated and the patient can eventually be weaned off oxygen (see section 12) (grade D).
U3: Most stable convalescent patients will eventually be stepped down to 2 L/min via nasal cannulae prior to cessation of oxygen therapy. Patients at risk of hypercapnic respiratory failure may be stepped down to 1 L/min (or occasionally 0.5 L/min) via nasal cannulae or a 24% Venturi mask at 2 L/min as the lowest oxygen concentration prior to cessation of oxygen therapy (grade D).
U4: Oxygen therapy should be stopped once a patient is clinically stable on low-concentration oxygen and the oxygen saturation is within the desired range on two consecutive observations (but the prescription for a target saturation range should remain active in case of future deterioration). It may be appropriate to alter the target range following senior review in patients with chronic cardiopulmonary disease who either have saturations <94% when stable or in whom it is deemed sensible to discharge from hospital with saturations <94% pending an outpatient oxygen assessment. Oxygen should also be stopped if the patient has come to the end of a written protocol of timed oxygen (eg, postoperatively) (grade D).
U5: Oxygen saturation on air should be monitored for 5 min after stopping oxygen therapy. If it remains in the desired range it should be rechecked at 1 hour (grade D).
U6: If the oxygen saturation and physiological ‘track and trigger’ score (eg, NEWS) is satisfactory at 1 hour, the patient has safely discontinued oxygen therapy. However, saturation and physiology should continue to be monitored on a regular basis according to the patient's underlying clinical condition (grade D).
U7:如果在停止氧疗时饱和度低于患者的目标范围,请重新启动使患者保持在目标范围内的最低浓度并监测5分钟。如果将饱和度恢复到目标范围,则继续在此水平进行氧疗,并在以后再次尝试停止氧疗,前提是患者保持临床稳定(D级)。
U8:如果患者需要以比以前更高的浓度重新启动氧疗以维持相同的目标饱和范围,则患者应进行临床检查以确定导致该恶化的原因(D级)。
U9:一些患者在安全停用氧疗后可能会出现偶发性低氧血症(例如,在轻微的运动后或由于粘液堵塞)。目标饱和度范围的持续处方将允许这些患者在需要时接受氧气,但是瞬时无症状的去饱和不需要校正(D级)。
V1:初级保健医疗中心应提供应急氧气,最好使用带有整体高流量调节器的氧气瓶。或者,必须使用配有高流量调节器(输送速度高达15 L / min)的氧气瓶,以便与储液罩(D级)一起使用。
V2:医疗保健组织应采取措施消除氧气管连接到不正确的壁式氧气出口或输送压缩空气或其他气体而非氧气的出口的风险。空气流量计应在不使用时从墙壁插座上拆下或用指定的出风口盖覆盖。如果使用双氧气出口(D级),应特别小心。
与氧疗的实际方面有关的良好实践要点
评估和立即氧疗
慢性低氧血症患者的临床恶化与其常规氧疗中氧饱和度下降3%或更多相关,通常应在医院进行血气评估。< 7kPa的PaO 2相当于SpO 2低于~85%。
如果有明确的哮喘病史或心力衰竭或其他可治疗的疾病,应根据每种疾病的指南或标准管理计划制定适当的治疗方案。
应持续监测血氧饱和度,直至患者稳定或到达医院进行全面评估。应向上或向下调节氧浓度以维持目标饱和范围。
在大多数紧急情况下,在没有正式处方或药物订单的情况下立即给予患者氧气。缺乏处方不应该排除在紧急情况下需要时给予氧气。然而,必须随后的书面记录是对每位患者给予氧疗(以与所有其他紧急治疗的记录类似的方式)。
全科医生(GP)或前往患者家中的急救人员应携带便携式脉搏血氧仪来评估低氧血症并指导氧气的使用,如果怀疑患有低氧血症或其他严重疾病,应拨打急救服务。
那些在农村或偏远地区作为紧急情况就诊的患者应考虑携带便携式氧气瓶作为其应急设备的一部分。
Oxygen alert cards for patients with hypercapnic respiratory failure
Patients with COPD (and other at-risk conditions) who have had an episode of hypercapnic respiratory failure should be issued with an oxygen alert card and with a 24% or 28% Venturi mask. They should be instructed to show the card to the ambulance crew and emergency department staff in the event of an exacerbation.
Oxygen alert cards with agreed content can be obtained via the BTS website.
The content of the alert card should be specified by the physician in charge of the patient's care, based on previous blood gas results.
The primary care team and ambulance service should also be informed by the hospital COPD team that the patient has had an episode of hypercapnic respiratory failure and carries an oxygen alert card. The home address and ideal oxygen concentration or target saturation ranges of these patients can be flagged in the ambulance control systems and information disseminated to ambulance crews when required.
When possible, out-of-hours services providing emergency primary care services should be informed by the hospital COPD team or by the primary care team that the patient has had an episode of hypercapnic respiratory failure and carries an oxygen alert card. Use of oxygen in these patients will be guided by the instructions on the alert card or by a patient-specific protocol which can be shared by hospital teams, the ambulance service and the primary care team.
W1: Registered nurses and others who dispense drugs in hospitals should sign the drug chart or electronic prescribing record at every drug round and check that the patient is receiving oxygen therapy. This is to check that the patient is within the target saturation and also to check whether weaning and discontinuation should be instituted (grade D).
W2: Most patients are prescribed an oxygen target range. If patients are on air at the time of the drug round, registered nurses should sign the drug chart using a code such as ‘A’ for air and the observation chart should also be filled in using the code A for air (see table 5 and figure 19) (grade D).
Working example of oxygen section for hospital prescription charts. *Saturation is indicated in almost all cases except for terminal palliative care.
W3: All patients should have their oxygen saturation observed for at least 5 min after starting oxygen therapy or for patients who require an increased concentration of oxygen and after oxygen therapy has been decreased or stopped (grade D).
W4: If the oxygen saturation is above the target saturation range and the patient is stable, the delivery system or oxygen flow rate should be modified to return the saturation to within the target range (grade D).
W5:目标饱和度为88-92%的患者应在30-60分钟内测量其血气。这是为了确保二氧化碳水平不会上升。该建议也适用于那些有发生高碳酸血症呼吸衰竭但在初始血气测量中具有正常PCO 2(D级)的人。
W6:氧饱和度在94-98%目标饱和度范围内的稳定患者如果没有高碳酸血症呼吸衰竭和酸中毒的风险,则不需要在30-60分钟内重复进行血气测量,并且可能不需要进一步的血气测量除非有进一步恶化,包括可能的高碳酸血症症状或体征(D级)。
W7:氧气治疗的稳定患者应该每天测量四次Spo 2和生理变量(例如,NEWS)(D级)。
W8:对于有严重疾病迹象的患者(例如,NEWS 7或以上),应持续监测血氧饱和度,并且患者可能需要在HDU或重症监护病房(D级)进行2级或3级护理。
W9:如果患者临床稳定并且氧饱和度在目标范围内,则应根据临床情况(D级)继续(或最终降低)治疗。
W10:如果饱和度低于所需范围,则应增加氧疗;如果饱和度高于所需范围,则应减少氧疗(并且最终在患者恢复时停止)(D级)。
W11:在新的氧浓度处理5分钟后,新的饱和度(和新的输送系统)和流速应记录在患者的观察图表上。每个变化都应该由接受过训练的临床医生记录,通过签署观察图表(只需要签署变更)(D级)。
W12:对于需要降低氧浓度(或停止氧疗)以维持所需目标饱和度(D级)的稳定患者,不需要重复血气测量。
W13:没有高碳酸血症呼吸衰竭风险的患者在氧浓度增加后并不总是需要重复血气测量。然而,患者需要临床检查以确定氧饱和度下降的原因(D级)。
W14:有高碳酸血症呼吸衰竭风险的患者(通常是那些目标范围为88-92%; 见表4)需要在氧疗增加后30-60分钟重复进行血气评估(以确保二氧化碳水平为没有上升)(D级)。
W15:对于没有高碳酸血症呼吸衰竭风险的患者,如果患者临床稳定且血氧饱和度保持在所需范围内,通过脉搏血氧仪监测就足够了(不需要反复输入血气),通常为94-98%(D级) 。
W16:如果患者的氧饱和度低于规定的目标范围,首先检查氧气输送系统和血氧计设备的所有方面是否有故障或错误(D级)。
W17:如果患者的血氧饱和度始终低于规定的目标范围,则应进行医学检查,并应根据商定的书面协议(D级)增加氧疗。
W18: If the oxygen saturation fails to rise following 5–10 min of increased oxygen therapy or if there is clinical concern following medical review, then blood gas measurements should be repeated (grade D).
X1: All clinicians prescribing oxygen should have appropriate training and access to written or electronic oxygen prescribing guidelines based on this national guideline (grade D).
(Training slides for doctors and nurses are available as online appendices 7 and 8 on the BTS website.)
X2: Every hospital should have a training programme to ensure that clinical staff are familiar with the hospital's oxygen administration policies. In view of the high number of adverse incidents related to oxygen therapy, it is recommended that all acute Trusts should include basic training in oxygen use in the mandatory training programmes for all clinical staff (grade D).
The key aim of this guideline is to make oxygen use in emergency and healthcare settings safer, simpler and more effective. Oxygen is probably the commonest drug used in the care of patients who present with medical emergencies. Prior to the publication of the first BTS guideline for emergency oxygen use in adult patients in 2008,2 ambulance teams and emergency department teams were likely to give oxygen to virtually all breathless or seriously ill patients and also to a large number of non-hypoxaemic patients with conditions such as ischaemic heart disease or stroke based on custom and practice. About 34% of UK ambulance journeys in 2007 involved oxygen use.3 This translated to about two million instances of emergency oxygen use per annum by all UK ambulance services, with further use in patients' homes, GP surgeries and in hospitals. Audits of oxygen use and oxygen prescription have shown consistently poor performance in many countries and most clinicians who deal with medical emergencies have encountered adverse incidents and occasional deaths due to underuse and overuse of oxygen.4–10
Historically, oxygen has been administered for three main indications of which only one is evidence-based. First, oxygen is given to correct hypoxaemia because severe hypoxaemia is clearly harmful to the human body. Second, oxygen has been administered to ill patients in case they might become hypoxaemic. Recent evidence suggests that this practice may actually place patients at increased risk if impaired gas exchange does actually develop (see section 6.3). Third, a very high proportion of medical oxygen was administered because most clinicians believed, prior to 2008, that oxygen can alleviate breathlessness in most circumstances. However, there is no good evidence that oxygen relieves breathlessness in non-hypoxaemic patients. There is evidence of lack of effectiveness or minimal effectiveness in mildly hypoxaemic breathless patients with COPD and advanced cancer (see sections 6 and 8.11.4).
Against this background, the Standards of Care Committee of the BTS established a working party in association with 21 other societies to produce an evidence-based guideline for emergency oxygen use in the UK. This led to the production of the 2008 BTS guideline for emergency oxygen use in adult patients which was the world's first guideline for emergency oxygen therapy.2 This guideline has been implemented throughout the UK and in many other countries leading to over 500 citations in the medical literature up to the end of 2016.
The purpose of the update to the 2008 guideline is to strengthen the evidence base of the previous guideline based on revised methodology (which meets criteria contained in the AGREE II instrument) and to extend the evidence base to the end of 2013.11 Additionally, the remit of the 2008 guideline has been broadened to cover several new aspects of oxygen use and a broader range of locations where oxygen might be used.
This guideline is mainly intended for use by all healthcare professionals who may be involved in emergency oxygen use. This will include ambulance staff, first responders, paramedics, doctors, nurses, midwives, physiotherapists, pharmacists and all other healthcare professionals who may deal with ill or breathless patients. Advice is also provided for first responders belonging to voluntary organisations or other non-National Health Service (NHS) bodies. Information based on this guideline is available on the BTS website for use in the following situations:
Hospital use
Primary care use
Ambulance use (supplemented by ambulance service guidance based on this guideline)12
Use by nursing staff and allied health professions.
指南的这些缩写版本包含与特定情况相关的关键建议和表格和图表。医疗保健组织可以下载“迷你指南”,以便在Trust内部网上使用,并为关键员工制作纸质版指南。
该指南针对院前和医院环境中的三大类成人患者以及姑息治疗等其他环境中的氧气使用情况:
重症患者,
低氧血症患者和有低氧血症风险的患者,
可能受益于氧气的非低氧血症患者(例如,一氧化碳中毒)。
儿科用氧:本指南仅适用于年龄> 16岁的患者。
氧气用于高海拔活动。
空中旅行时的氧气使用。
水下潜水和潜水事故。
在动物实验中使用氧气。
HDU中的氧气使用。
ICU中的氧气使用。
院内3级转学。
高压氧。
呼吸支持技术包括气管插管,有创通气和NIV(包括CPAP)。
由于任何原因患有家用氧气的患者自行使用氧气。
在家里持续照顾低氧血症患者。
证据审查方法已从NICE方法改为BTS NICE认可的指南生产流程,该流程基于苏格兰校际指导网络(SIGN)方法,并遵循AGREE方法(参见第1节)。
该指南的证据基础已更新至2013年8月(并延长至2016年底,以供关键参考)。2008年的所有建议都没有受到新证据的挑战,但许多现有建议都得到了新信息的支持。自2008年以来,已有许多观察性研究,但很少有与该指南直接相关的随机试验。
The new guideline covers not just emergency oxygen use but most oxygen use in healthcare settings. It also covers short-term oxygen use by healthcare workers outside of healthcare settings but domiciliary oxygen use by patients is covered by the BTS guideline for home oxygen use in adults.13
The present guideline includes the following new topics and settings which have been requested by guideline users:
Postoperative and perioperative care including PCA,
Endoscopy and other procedures requiring conscious sedation,
Palliative care settings including hospices,
Use of helium–oxygen mixtures (Heliox) and nitrous oxide/oxygen mixtures (Entonox),
Use of CPAP,
Use of oxygen by healthcare professionals in patients' homes,
Use of oxygen by voluntary rescue organisations and other non-NHS first responders,
High-flow nasal cannulae (HFNC).
The structure and format of the guideline has been changed since 2008:
The 2008 guideline was published as a supplement in Thorax.2 Additional educational materials and other resources including audit tools were made available on the BTS website. The new guideline exists in two complementary formats.
A concise guideline which contains recommendations and good practice points is published in BMJ Open Respiratory Research.
The full guideline including evidence review, physiology overview, illustrations and references is published in this edition of Thorax and is available on the BTS website http://www.brit-thoracic.org.uk.
This guideline is based on the best available evidence concerning oxygen therapy. However, a guideline can never be a substitute for clinical judgement in individual cases. There may be cases where it is appropriate for clinicians to act outwith the advice contained in this guideline because of the needs of individual patients, especially those with complex or interacting disease states. Furthermore, the responsibility for the care of individual patients rests with the clinician in charge of the patient's care and the advice offered in this guideline must, of necessity, be of a general nature and should not be relied on as the only source of advice in the treatment of individual patients. In particular, this guideline gives very little advice about the management of the many medical conditions that may cause hypoxaemia (apart from the specific issue of managing the patients' hypoxaemia). Readers are referred to other guidelines for advice on the management of specific conditions such as COPD, pneumonia, heart failure, etc. Some of these disease-specific guidelines may suggest slightly different approaches to emergency oxygen therapy whereas the present guideline aims to provide simple all-embracing advice about oxygen therapy.
The need for a national guideline for emergency oxygen use was recognised by the BTS Standards of Care Committee in 2003. A working party was established with representatives from a wide range of professions involved in oxygen therapy and a lay representative. The original group was expanded in 2006 because it became clear that the development and implementation of a national guideline would require input from a very wide range of professional groups. This group agreed the remit of the 2008 guideline and a series of key questions which were addressed within the 2008 guideline.2 The group membership was expanded further and the remit was expanded for the 2016 update of the guideline. A full list of guideline group members is provided in annex 1. The methodology for the 2016 guideline adheres to the BTS Guideline Production Manual 2014 which is aligned to the AGREE criteria for guideline production.11 ,14
MEDLINE对“氧气”的搜索产生了超过25万次“点击”,其中大部分都与本指南无关。出于这个原因,BTS委托约克大学的评论和传播中心和卫生经济学中心根据2008年指南中使用的文献检索策略进行定制的文献检索。搜索策略在BTS网站(http://www.brit-thoracic.org.uk)的在线补充附录1中有详细说明。
缺氧/低氧血症的危害是什么(即人体会发生什么)?
什么水平的低氧血症对所有患者(甚至健康成人)都有危险?
什么水平的低氧血症对弱势群体(如缺血性心脏病,中风,老年人)有危险?
用以下关键词重复上述搜索:老年人,中风,心肌梗塞,心力衰竭,COPD,创伤,肾衰竭。
高碳酸血症/高碳酸血症的相同问题:
搜索“高碳酸血症”并结合暗示有害结果(死亡/组织损伤/脑损伤/昏迷)的术语。
什么级别的高碳酸血症对所有患者都有危险?
什么级别的高碳酸血症对弱势群体是危险的(如上所述)?
呼吸性酸中毒的相同问题:
搜索“呼吸性酸中毒”并结合暗示有害结果(死亡/组织损伤/脑损伤/昏迷)的术语。
什么级别的呼吸性酸中毒对所有患者都有危险?
什么级别的呼吸性酸中毒对弱势群体有危害(如上所述)?
如何评估低氧血症(临床,EWS系统,血氧测定,动脉和毛细血管血气)。
如何评估高碳酸血症/高碳酸血症。
使用氧气缓解症状性呼吸困难。
在急性COPD中使用氧气。
在急性哮喘中使用氧气。
在肺炎中使用氧气。
使用氧气治疗肺栓塞。
在创伤中使用氧气。
在心力衰竭中使用氧气。
在心肌梗塞和不稳定的冠状动脉综合征中使用氧气。
在心绞痛中使用氧气。
对于具有较少常见病症的其他患者使用氧气被单独搜索(例如,CF,肌营养不良,运动神经元疾病,严重脊柱后凸,过敏反应,过度换气)。
Oxygen carriage in transport (practical issues; safety issues).
Oxygen delivery systems in ambulances.
Prescription of oxygen.
Local hospital guidelines for oxygen use.
Oxygen delivery systems in hospitals and other healthcare and emergency settings.
Advantages/disadvantages of each delivery system (Venturi masks, simple face masks, nasal cannulae, high-flow masks such as non-rebreathing reservoir masks). Use of oxygen-driven nebulisers.
Use of CPAP.
Use of ‘alert cards’, alert bracelets or similar hazard warning systems for patients who are known to be at risk of hypercapnia.
The search strategy and guideline methodology for the 2008 guideline are described within the original guideline.2 The remit of the guideline was widened for this update. Significant new areas include the use of oxygen during conscious sedation procedures, the non-emergency use of oxygen in healthcare settings and the use of CPAP, Heliox and oxygen–nitrous oxide mixtures. The methodology used for the current guideline was based on SIGN methodology as outlined in the BTS Guideline Production Manual 2014.11 ,14 ,15
The 2008 guideline had used NICE levels of evidence so all searches were rerun in November 2011 and again in August 2013. All abstracts retrieved by the literature search were screened by pairs of members and reprints of all relevant papers were obtained. Members of the Guideline Development Group worked in pairs to assign a SIGN level of evidence to all of the papers that were judged to be relevant to the guideline (see tables 6 and 7). Further references were obtained from the group's personal literature collections and from the references contained within the papers which the search yielded and by focused literature searches by members of the guideline group. The group continued to monitor the literature up to the end of 2016 for important new publications or very high-quality abstracts from international meetings that were thought to be relevant to this guideline.
The group was divided into subgroups to work on each chapter of the guideline. Contributions by each member of the group are acknowledged in annex 1. The Guideline Development Group corresponded by email on a regular basis to discuss the evidence and to update the guideline and its key recommendations over the course of 2011–2016. Oxygen therapy is unusual insofar as there are very few published trials where different levels of oxygen therapy have been compared in randomised studies which reported clinically relevant outcomes. Most advice concerning oxygen therapy is based on expert opinion guided by extrapolation from non-interventional studies that do not directly address guideline questions. For this reason, most of the recommendations in this guideline are at grade D and it is hoped that the deficiency of relevant evidence will stimulate researchers to conduct randomised trials of oxygen therapy. However, the fact that a recommendation is graded as ‘grade D’ due to lack of evidence does not imply that the recommendation is not important of that there is any uncertainty as to the correct course of action. For example, it would never be ethical to undertake a randomised controlled trial (RCT) of oxygen therapy in severe hypoxaemia, so the advice to use oxygen to correct severe hypoxaemia will always be a grade D recommendation but it is one of the most important recommendations in this guideline.
整个小组的会议于2011年11月和2012年9月举行。更新的指南由BTS标准护理委员会于2014年9月,2015年3月,2015年9月和2016年6月进行了审查。该指南通过电子邮件讨论进一步完善。这个委员会。该草案于2015年12月7日至2016年1月18日期间通过BTS网站提供,为期6周,供公众和利益相关方参与,并邀请评论。该文件草案当时已发送给两名同行评审员。修订后的文件随后于2016年10月提交给英国胸科协会进行最终批准,并获得其他利益相关方协会和学院的认可。
2008年英国范围内的传播之前,索尔福德皇家大学医院和绍森德大学医院试行了2008年指南(目标饱和度范围等)的原则。2008年英国医院的氧气使用基线审计于2008年开始实施。该指南和流程每年由BTS每年审核一次,这些审核除了对每家医院的流程进行审核外,还监控指南政策的实施情况。16
成功实施政策的主要特点是:
信托范围内对商定的医院政策的介绍。
英国的每家医院都有一个或多个“氧气冠军”来实施和审核当地氧气的安全使用(见第14.6节)。
为医生,护士和其他氧气使用者提供本地入职培训和教育计划。
介绍处方图和患者观察图表,以促进氧疗的标准化(图19)。根据BTS网站上的模型文件制作和实施详细的医院氧气政策(见在线补充附录)。
使用标准图表来指导氧气的处方和给药(图19)。
网络附录7-11中的教育材料和讲座演示已在英国广泛使用,并得到了每家医院氧气冠军的反馈。
该指南将在出版后5年内由英国胸科协会进行审查。
指南小组的所有成员都根据BTS政策作出了感兴趣的声明,并且可以应BTS的要求获得进一步的细节。
正常血液中的氧气和二氧化碳含量。
正常氧饱和度(SaO 2)和正常血液pH值。
低氧血症,缺氧,高碳酸血症,酸中毒,呼吸衰竭的定义。
氧以两种形式在血液中传输:小的和可忽略的量溶解在血浆中,并且大部分与血红蛋白结合并递送到组织。运动期间需氧量和氧气输送量增加,休息和睡眠时减少。
The human lung delivers oxygen to the blood and removes carbon dioxide. Several mechanisms exist to regulate breathing in such a way that both gases are maintained within quite a narrow range, although carbon dioxide levels are more tightly regulated than those of oxygen.
As there is a fixed amount of haemoglobin circulating in the blood, the amount of oxygen carried in the blood is often expressed in terms of how saturated with oxygen the circulating haemoglobin is. This is what is meant by ‘oxygen saturation level’. If this is measured directly from an arterial blood sample, it is termed SaO2. If it is measured from a pulse oximeter it is termed SpO2. Alternatively, one can measure the PO2 of the blood (PaO2), known as the ‘partial pressure of oxygen’ in the blood. This measurement can be expressed in kilopascals (kPa; normal range 12.0–14.6 kPa) or in millimetres of mercury (normal range 90–110 mm Hg for young adults).17 The precise normal ranges for oxygen saturation and PO2 are difficult to determine accurately due to a lack of data from the ‘normal’ population, that is, non-hospitalised healthy participants.
A US observational study of nearly 900 asymptomatic patients in the emergency department showed the median SpO2 value to be 99% with SpO2 values <97% occurring in 5.7% of the study group.18 However, the study group were young (median age 38) and predominantly African-American, so these data are not generalisable to the UK population.
Another North American study measured blood gases and SpO2 at sea level in 96 healthy individuals aged between 18 and 81.17 They found that for adults 2SD range for SaO2 is ∼94–98% at sea level but this may decline gradually with advancing age (table 8).
Mean (SD) PaO2 (kPa and mm Hg) and SaO2 (%) values (with range)
A much larger observational study of over 37 000 patients admitted to four acute medical admissions units across the UK19 found that median SpO2 was 98% for young adults aged 18–64 years (IQR 97–99%). For adults aged ≥65 years the median saturation was 96% with IQR 95–98% (table 9). While the authors of this study recommend setting a normal range of 96–98%, their study excluded nearly 20% of patients who were receiving oxygen, many whom were likely to have a SpO2 in the lower end of the normal range. In further considering these study results, it is of note that the PaO2 is 0.8 kPa (6 mm Hg) lower in the supine position than in the upright position and most emergency measurements are made in the supine position.20
Ranges, mean, SD, median and IQR values for SpO2 (%) where measurements were made with the patient receiving air for age ≥18 years (n=37 299) from Smith et al19
The mean SaO2 may be lower in older people than in young adults. However, it is difficult to dissociate the effects of advancing age from the effects of the diseases that become commoner in old age. Some papers have reported a fall in the blood PaO2 in older participants. Indeed a fall in SpO2 in patients >65 was demonstrated in Crapo and Smith's studies, and the former study shows a decreasing PaO2 with age. However, others have failed to confirm this observation.21–23 The mean SaO2 in seated adults aged >64 years in one published study was 95.5% compared with 96.9% in adults aged 18–24 years, and the SD was wider in the older age group with a 2SD range of 92.7–98.3% (tables 8 and 9).17 The mean (SD) SaO2 for recumbent healthy men aged >70 years in another study was 95.3% (1.4%) giving a 2SD range of 92.5–98.1% for men of this age.21 The mean (SD) SaO2 was 94.8% (1.7%) for recumbent healthy women aged >70 years with a 2SD range of 91.5–98.2%. The authors of this study did not observe any age-related decline in SaO2 beyond the age of 70 years. The mean SaO2 in this study of ∼95.0% for recumbent healthy men and women aged >70 years was below the normal range for seated healthy young adults. The mean PaO2 in older participants in this study was 10.3 kPa for men and 9.8 kPa for women, which is lower than two other studies which reported mean PaO2 values of 11.2 kPa and 11.1 kPa in healthy older participants.22 ,24 Some of these differences are probably due to participant selection, but there may also be variations in the results obtained by different blood gas analysers.25
来自Salford和Southend的320名稳定住院患者的未发表的审计的进一步数据显示,年龄> 71岁的患者中,平均(SD)SpO 2为96.7%(1.77%; 2SD范围95.2-100%) R O'Driscoll,A Davison,L Ward,个人通讯)。这些数值是在2008年英国医院通过脉搏血氧测定法测量的,更有可能代表英国老年人群中脉搏血氧测量的预期正常范围。随着年龄,性别和姿势的变化使得难以给出适用于可能需要氧疗的所有成年人的精确目标范围,但指南制定委员会认为94-98%的目标范围将达到正常或接近 - 正常的SpO 2 / SaO 2 对于英国的大多数成年人而言,将避免任何临床上显着的低氧血症的风险。
虽然吸入空气中的氧气百分比恒定在21%并且不随海拔高度而变化,但是在较高海拔处的大气压力下降会降低吸入氧气的分压。在给定高度的SaO 2随年龄,性别,种族和适应高度的程度而变化。例如,居住在西藏海拔约4000米的所有年龄段的3812人的样本平均SaO 2仅为88.2%,但安第斯山脉居民的SaO 2比居住在西藏的西藏人高约2.6%。相同的高度。26 ,27然而,海拔低氧血症的生理学与海平面低氧血症的生理学非常不同,例如,呼吸机改变通常导致动脉CO 2水平显着下降。数百万人生活在这些海拔高度,其中SaO 2值会引起海平面的关注。玻利维亚的拉巴斯市平均海拔3600米,人口约150万。珠穆朗玛峰(8848米)的登山者SaO 2可低于55%。28突然暴露在海拔4000米以上的海拔高度可导致山区疾病,高原肺水肿和高原脑水肿。长期暴露于高海拔地区(或因任何其他原因导致低氧血症)可导致肺动脉高压。
如果血氧水平甚至几分钟(例如,在心脏停搏期间)降至极低水平,将发生组织缺氧和细胞死亡,尤其是在脑中。在严重低氧血症期间,大脑似乎是最脆弱的器官; 脑功能障碍是缺氧的首要症状,脑损伤是心脏骤停幸存者和其他严重低氧血症的最常见的长期并发症。即使在健康的参与者中,突然暴露于低于约80%的低SaO 2也会导致意识改变。患有严重疾病或慢性器官损害的患者的其他器官很可能在氧气水平高于80%时易受缺氧组织损伤的风险。
大多数专家强调了对于大多数急性病患者,将SaO 2保持在90%以上的重要性。29-32然而,导致细胞损伤的缺氧程度尚未确定,可能不是绝对值。例如,健康的老年人休息时的SaO 2值低于年轻人。许多患有慢性肺病,先天性紫绀型心脏病或慢性神经肌肉疾病的患者的氧饱和度大大低于正常范围,即使临床稳定。
然而,尽管慢性低氧血症患者在临床稳定状态下可能耐受异常低的SaO 2,但在组织需氧量增加时(例如,败血症,创伤等)急性疾病期间,这些静息氧水平可能不足以进行组织氧合作用。肺炎,头部受伤;见第8节)。
Acute hypoxaemia with SaO2<90% and sometimes <80% is seen in many acute illnesses such as pneumonia and heart failure and it is likely that the clinical manifestations of hypoxaemia in illness would be similar to those of experimental hypoxaemia in hypobaric chambers (impaired mental function followed by loss of consciousness). However, the clinical manifestations of the illness itself make it difficult to identify which symptoms and signs are due to hypoxaemia. Pure hypoxaemia, as seen in hypobaric chambers and at altitude, does not seem to cause breathlessness in resting participants. Patients with chronic diseases such as COPD, lung fibrosis, neuromuscular disorders or congenital heart disease may routinely attend outpatient clinics with SaO2 levels well below 90% even at a time when their disease is stable. In an emergency, a clinician who was not familiar with such a patient (when stable) might interpret the low saturation as having occurred acutely and aim to achieve an oxygen saturation that was well above the patient's usual oxygen saturation level. Many such patients would qualify for long-term oxygen therapy. The UK COPD guideline recommends a threshold of 7.3 kPa (55 mm Hg) below which most patients with COPD will benefit from long-term oxygen therapy (equivalent to a SaO2 of about 88–89%) and an PaO2 threshold below 8.0 kPa (60 mm Hg) for patients with established cor pulmonale and some other subgroups.1
Healthy participants in all age groups have greater variation in SaO2 when sleeping than while awake. A study of 330 people referred to a sleep laboratory with normal results of overnight polysomnography (patients with cranial facial or neurological abnormalities or previously diagnosed pulmonary disease were excluded) showed that desaturation routinely occurred with a mean (SD) minimum SaO2 or ‘nadir’ of 90.4% (3.1%) during the night (2SD range 84.2–96.6%).33 The mean (SD) overnight SaO2 ‘nadir’ was 89.3% (2.8%) for participants aged >60 years.33 In this study, participants aged 20–30 years spent 10% of the night with SaO2 levels below 94.8% and half the night below 96.3%, and those aged 60 years spent 10% of the night below 92.8% and half the night below 95.1%. Furthermore, the authors of this study excluded obese patients with any features of sleep apnoea or hypopnoea because these patients are known to desaturate to very low levels during sleep (often below 70%). The variation in SaO2 during sleep is exaggerated by alcohol and by sedative drugs. This makes it difficult to evaluate a ‘spot reading’ of SaO2 on a sleeping participant. It is suggested that SaO2 measurements of sleeping participants should be interpreted with caution and ideally observed for a few minutes to see if the participant has got sustained hypoxaemia or just a transient normal ‘nocturnal dip’.
Oxygen saturation in acute and chronic disease is discussed in section 3.1.4.
Evidence statements (see recommendations A1–A2):
Normal daytime haemoglobin SaO2 is 96–98% in young adults in the seated position at sea level but the lower limit falls slightly with age and is ∼94–98% in adults aged >70 years (evidence 2+).
All participants have transient dips in oxygen saturation at night with a mean nadir of 90.4% (2SD range 84.2–96.6%) in healthy participants in all age groups (evidence level 3).
The reference range for arterial carbon dioxide tension (PaCO2) is 4.6–6.1 kPa (34–46 mm Hg) for healthy adult men aged 18–38 years.34 Although this study was undertaken in 1948, it is consistent with the clinical experience of the guideline group members and with most modern reference values for PaCO2. Although different laboratories and textbooks give slightly different reference values, all are within 0.2 kPa of the above reference range. Any value of PaCO2 of >6.1 kPa (45 mm Hg) should be considered abnormal, but values up to 6.7 kPa (50 mm Hg) may be obtained by breath holding.35
低氧血症是指血液中的低PO 2或氧分压(PaO 2)。出于实际原因,还可以测量低氧血症与氧合血红蛋白饱和度的关系。在成人中,正常范围受年龄和合并症的影响,健康成人的正常范围在3.1.1节中给出。患者变得低氧血症的精确水平是值得商榷的。有人可能会争辩说,任何低于正常下限的饱和度都会构成低氧血症。不同的作者将低氧血症定义为(1)的SaO 2 <94%; (2)<92%; (3)<90%; 或(4)PaO 2 <60 mm Hg或8 kPa。4 ,36-38谁研究过这方面的大多数作者都定义为低氧血症氧分压2<60 mm Hg(8 kPa)或SaO 2 <90%。39没有已知的低氧组织损伤风险高于此水平,其他关键重症监护指南设定为90%,低于SaO 2不应允许降至最低值。31 ,32
缺氧:当氧供应不足以满足特定隔室中的氧需求(例如,肺泡或组织缺氧)时,发生缺氧。组织缺氧可以细分为四个主要原因:低氧血症,贫血,停滞或组织毒性。氧疗可能只能纠正由于低氧血症引起的缺氧,需要考虑改善向组织输送氧气的其他方法。
低氧血症缺氧:由于氧分压降低,血液中的氧含量低时,存在低氧血症(有时也称为缺氧缺氧)。这在高海拔时自然发生,或者发生在右向左分流,通气 - 灌注(V / Q)不匹配,肺泡通气不足或扩散损伤之后。
1型呼吸衰竭,定义为PaO 2 <8 kPa或60 mm Hg(相当于约90%的SaO 2),具有正常或低PaCO 2水平是由于缺氧缺氧。
贫血缺氧:贫血缺氧是由于可用于氧运输的血红蛋白水平降低所致。尽管患者可能不是低氧血症(具有正常的PaO 2和SpO 2),但血液中氧含量的降低可能导致组织缺氧。一氧化碳中毒还可能通过削弱血红蛋白结合氧的能力而产生一种贫血性缺氧形式,从而降低携氧能力。
停滞缺氧:由于血流不足(全球或区域性),停滞缺氧是组织中低水平的氧气。如果一个人长时间暴露在寒冷的温度下,这种情况可能发生在四肢,并且它是组织中坏疽的原因,在严重的外周血管疾病中被剥夺了血液。在低心输出量状态下可能发生停滞缺氧。
组织毒性缺氧:组织毒性缺氧是由于正常细胞代谢的中断,组织不能使用氧气。最明显的例子发生在氰化物中毒过程中,这会损害细胞色素的功能。越来越多的人认为,尽管有足够的氧气输送,线粒体功能障碍可能导致脓毒症的氧气使用减少。这也被称为“细胞病变性障碍”。40
高氧和高氧血症:高氧和高氧血症是上述术语的对应物,并且在该指南中分别指的是隔室中的高氧含量和血液中的高PO 2。如上所述,出于实际目的,血液中的PO 2通常被测量为氧合血红蛋白饱和度。此外,本指南的重点是为各种条件提供目标饱和度,但应注意的是,在约16 kPa(120 mm Hg)的PaO 2以上,氧合血红蛋白饱和度显然不会从100%变化,但进一步增加的影响在某些情况下,如COPD ,PaO 2可能很重要。这将在第5节和第6节中进一步详细讨论。
当PaCO 2高于正常范围4.6-6.1 kPa(34-46 mm Hg)时会出现高碳酸血症,即使氧饱和度在正常范围内,高碳酸血症患者也会出现2型呼吸衰竭。一项针对单一医院的3524份血气样本的研究发现,27%的人患有2型呼吸衰竭,而6%的样本患有1型呼吸衰竭。这些样品中有41%表现出高氧(PaO 2 > 16kPa)。41排除急诊科样本(其中许多是静脉)并排除重复样本(COPD患者常见),8.5%的样本显示1型呼吸衰竭,22.7%显示高碳酸血症。42 Hypercapnia was commoner than pure hypoxaemia on surgical wards and critical care areas as well as on medical wards.
Acidosis: Acidity in any fluid is determined by the concentration of hydrogen ions [H+], and this is normally regulated between 35 and 45 nmol/L. Acidity is more often expressed in terms of pH where pH=−log10[H+]. The normal pH range of the blood in humans is between 7.35 and 7.45 units. Acidosis is defined as a pH<7.35 ([H+]>45 nmol/L) and alkalosis is defined as a pH>7.45 ([H+]<35 nmol/L). Acidosis can be caused by respiratory or metabolic disorders.

Carbon dioxide (CO2) can combine with water (H2O) to form carbonic acid (H2CO3) in the blood which, in turn, dissociates to bicarbonate (HCO3−) and a hydrogen ion (H+). Acute respiratory acidosis occurs if the pH of the blood falls below 7.35 ([H+]>45 nmol/L) in the presence of a raised CO2 level. If respiratory acidosis has been present for more than a few hours, the kidney retains bicarbonate to buffer the acidity of the blood and, over hours to days, this may be sufficient to produce a normal pH. This situation (high PaCO2 with high bicarbonate and normal pH) is known as ‘compensated respiratory acidosis’. This situation is common in patients with chronic severe but stable COPD, but they may have an additional acute rise in PaCO2 during an acute exacerbation giving rise to ‘acute on chronic’ respiratory acidosis despite their high bicarbonate level. This happens because the bicarbonate level was equilibrated with the previous CO2 level and is insufficient to buffer the sudden further increase in CO2 level that may occur during an exacerbation of COPD. Respiratory acidosis is common in clinical practice. Plant et al43 showed that about 20% of patients with AECOPD requiring hospital admission have respiratory acidosis.
Metabolic acidosis: This can be caused by failure to excrete acid produced by the body's normal metabolic processes (eg, during renal failure) or by increased production of acid from abnormal metabolic conditions such as diabetic ketoacidosis. Alternatively, it may result from direct loss of bicarbonate from the kidney or gut (eg, during chronic diarrhoea). In all forms of metabolic acidosis, there is a low blood bicarbonate level, either due to loss of bicarbonate or due to buffering of excess acid by bicarbonate which is excreted as CO2. A common cause of metabolic acidosis is lactic acidosis caused by tissue hypoxia. This may result from decreased oxygen delivery such as occurs in hypoxaemia, or low cardiac output states or conditions such as sepsis where oxygen consumption is impaired in the face of adequate oxygen delivery. In health, metabolic acidosis will occur at peak exercise where oxygen delivery is insufficient to meet demand.
A full understanding of blood gas physiology in the body requires a detailed understanding of the anatomy, physiology and biochemistry of respiration and gas exchange. It is recognised that most readers of this guideline may not have had full training in all of these specialties, so this physiology section contains a brief overview of basic principles for the non-specialist reader. The rationale for targeted oxygen therapy is discussed in detail in section 6.
Oxygen is transported in the blood in two forms: a small and negligible amount is dissolved in the plasma and the majority is bound to the haemoglobin molecule. As there is a fixed amount of haemoglobin circulating in the blood, the amount of oxygen carried in the blood is often expressed in terms of how saturated circulating haemoglobin is with oxygen (SO2).
As discussed in section 3.1 the precise normal SaO2 in healthy adults at sea level is not known. However, it is within a narrow range of about 95–98%. This means that almost all of the oxygen-carrying capacity of haemoglobin in the blood is used when the SaO2 is in the normal range. Therefore, giving supplemental oxygen to a healthy young person will increase the saturation level only slightly from about 97% to 99% or a maximum of 100%, thus producing only a very small increase in the amount of oxygen made available to the tissues.
即使在健康的参与者中,突然暴露于低SaO 2水平(低于约80%)也可导致精神功能受损。大脑是缺氧的不良反应最敏感的器官,但患有严重疾病的患者的其他器官可能在高于此范围的氧气水平下易受低氧组织损伤的风险。大多数专家强调将大多数急性病患者的SaO 2保持在90%以上的重要性。29-32本指南建议理想的目标饱和度范围为94-98%。该范围反映了英国成年人的正常范围,其安全范围大于上述90%的阈值。
氧气从肺部的吸入空气进入血液并传递到组织。如果PaO 2(局部压力)落入血液中,则由颈动脉体内的受体(由颈部的颈动脉供给)感知,并且刺激通气以增加进入肺部的氧气量,从而增加血液中的氧气量。 。肺具有将血流从通风不良的区域转移的能力,使得从身体返回的血液可以有效地补充氧气并且还清除二氧化碳。这通过称为“缺氧血管收缩”的过程发生,其中局部低PO 2在肺部空气空间引起血管收缩,因此将血液转移到肺部区域,通风良好。这种机制对于肺来说是独特的:大脑,心脏和肾脏等其他器官的循环会因缺氧而血管扩张,以促进更多的血液流向缺氧的区域。
如果血液的携氧能力低,例如贫血,则由产生激素促红细胞生成素的肾脏检测,以刺激红细胞生成; 但是,这个过程会持续数天到数周。由于循环的目标之一是向身体组织输送氧气,心脏也会通过增加其输出来响应低氧水平,从而增加“氧气输送”。这发生在几秒钟内。
低氧血症,低PaO 2,可以由多种机制引起。它在高海拔时自然发生,或者可能发生在V / Q不匹配之后,也就是由于肺部区域通气不良或由于肺部严重疾病期间肺内气体交换异常导致肺部缺氧,血管收缩不足能够弥补这种不匹配。这种形式的低氧血症最容易用氧疗法治疗。氧气治疗在组织缺氧的其他原因中效果较差,包括贫血,其中携带能力低或者血红蛋白的携带能力已被有毒物质降低,因为氧气可用性不是这些条件的限制特征。例如,尽管在肺部和血液中具有正常水平的氧气,但一氧化碳阻止氧气与血红蛋白结合。
二氧化碳是人体新陈代谢的产物。它通过从血液转移到肺部的肺泡然后从肺部呼出而从体内清除。它也通过肾脏排出,其中CO 2和水形成碳酸,然后碳酸离解成H +和HCO 3 -。以与氧类似的方式,血液中的二氧化碳水平由化学传感器(在颈动脉体和脑干中)控制。
二氧化碳在血液中高度溶解,以三种形式携带:碳酸氢盐(70-85%),溶解二氧化碳(5-10%)和血红蛋白结合(10-20%),百分比根据是否有所不同而不同是动脉或静脉血。由于二氧化碳载体不受诸如血红蛋白的载体分子的限制,因此不表示为饱和。因为其载体大致与生理范围内血液中二氧化碳的分压(气体张力)成比例,所以二氧化碳运输通常用其分压表示。正常范围是4.6-6.1 kPa或34-46 mm Hg。
Increased levels of carbon dioxide will stimulate ventilation, thus increasing clearance from the lungs and therefore from the bloodstream. However, this mechanism is less effective in some respiratory diseases such as COPD where increased airway resistance and respiratory muscle weakness can restrict this response, or where loss of the hypercapnic drive (eg, during chronic hypercapnia or severe brain injury) also depresses the ventilatory response. Hypercapnia will occur when there is decreased effective or ‘alveolar’ ventilation for any reason. Safe elimination of carbon dioxide is an important physiological process in the body to maintain pH.
Too little oxygen can give rise to increased respiratory work to combat the hypoxaemia and, potentially, organ dysfunction and failure. However, too much oxygen can also be harmful in some situations especially to some vulnerable patients with COPD, chest wall deformities or muscle weakness.
Studies have shown that between 20% and 50% of patients with AECOPD or with obesity-hypoventilation syndrome (OHS) are at risk of carbon dioxide retention if they are given an excessively high concentration of oxygen.43–47 If high concentrations of oxygen are given to these patients, the oxygen level in the blood will rise but the level of carbon dioxide will also rise. This can cause acidosis and, when severe, coma. In the past it was thought that the main problem was that these patients were dependent on the stimulus of a low blood oxygen level—called ‘hypoxic drive’—to stimulate breathing. It was thought that giving oxygen would cause a rise in the carbon dioxide level by simply reducing the stimulus to breathe due to ‘lack of hypoxic drive’. However, studies have shown that the mechanisms for carbon dioxide retention are far more complex than this simple model suggests.48–50
Oxygen-induced hypercapnia in patients with AECOPD can be avoided by giving targeted lower concentration oxygen therapy to vulnerable patients and aiming for a target range of 88–92%51 (see table 3 and recommendation A3).
One might ask why one should not aim for a SaO2 of 100% (hyperoxaemia) in all acutely ill patients. This policy has been shown to worsen outcomes in vulnerable patients with COPD and chest wall problems, but there is also a potential for harm to other patients.
While the administration of oxygen to the hypoxaemic patient leads to an increase in PaO2 which leads to favourable physiological effects and ultimately the prevention of cell death, administering oxygen to the non-hypoxaemic patient has other physiological effects which are not widely appreciated, although how important these are clinically is not clear in most cases. These potentially adverse effects include direct pulmonary toxicity, coronary vasoconstriction, decreased cardiac output, increased free radical generation and the potential to delay the recognition of physiological deterioration due to the masking of any desaturation. These risks are discussed in detail in section 6.
For this reason, the guideline group recognises the importance of a physiological target saturation range to guide staff to administer oxygen in a concentration to treat hypoxaemia without the risks of hyperoxaemia. As alluded to in section 3, some patients are chronically hypoxaemic and tolerate lower than normal saturations. The only RCT of oxygen therapy in patients with AECOPD randomised patients to receive high-concentration oxygen therapy versus titrated oxygen to keep SpO2 88–92% in the prehospital setting.51 Mortality was significantly lower in patients receiving titrated oxygen rather than high-concentration oxygen. This study highlights the importance of maintaining a target saturation when administering oxygen to this and other high-risk groups.
由于氧疗的目的是增加向组织的氧气输送,而不仅仅是为了增加血液携带的氧气,必须记住,可能存在需要纠正的其他生理紊乱,以增加氧气输送,例如低心输出量和严重贫血。例如,改善这些因素将比向患者施用氧气更多地改善氧气输送,其饱和度为90%,这最多将使输送增加10%。除了优化从肺部到组织的氧气输送(DO 2)之外,重要的是治疗可能影响肺部自身输送氧气的问题,例如上呼吸道阻塞,支气管收缩和肺水肿(记住'ABC'复苏 - 气道,呼吸,循环)。
自这些指南首次发表以来,已经开展了进一步研究,研究氧疗法在慢性肺病以外的疾病中的作用。这些已经证明了高氧的潜在风险,将在后面的章节中讨论。尽管有这些新数据,仍然没有足够的数据来确定健康成人的确切目标范围。指南组成员之间的共识是,对于急性病患者,正常或接近正常的SaO 2范围为94-98%,除了目标饱和度范围为88-92的高碳酸血症呼吸衰竭风险者外应使用%(见建议A1-A5)。
本节是围绕氧疗的生理问题的更深入的描述。本指南第6部分中的建议1-5将从本节和第4节中的氧气生理学简要概述开始。
神经心肺轴设计用于优化全球氧输送和二氧化碳清除,局部组织血管床负责血流分布。
DO 2由以下等式表示:
其中CaO 2是动脉血的氧含量,Q是心输出量。CaO 2是溶解在血液中的氧气和血红蛋白携带的氧气量之和。氧在血液中的溶解度非常低,因此CaO 2很大程度上取决于血红蛋白的总量和与氧结合的比例; 而这又取决于血红蛋白的饱和度。
图3显示了肺动脉,肺泡和室内空气以及肺静脉循环中氧气和二氧化碳的水平,其直接导致动脉循环。混合的全身静脉血的PaO 2从肺动脉的末端(约6kPa或45mmHg)显着上升至约16kPa(120mmHg)至肺毛细血管末端。然而,由于肺不是由灌注和通气匹配的肺泡毛细血管单元均匀组成,因此PaO 2在较大的肺静脉中较低(13kPa,100mmHg)。这在下面更详细地解释。二氧化碳的梯度更加平缓,从静脉系统和肺动脉中的约7kPa(52mmHg)下降到肺静脉和动脉系统中的约5kPa(37mmHg)。
对低氧血症的通气反应。当针对氧合血红蛋白(实线)饱和度绘制时,该关系是反向线性的,但是当针对动脉PO 2(虚线)绘制时,该关系是反指数的。PO 2,氧气张力。
在直立位置,通气和灌注在肺底部最大。由于肺的重量和胸腔内压力较低,肺部在基部受压最大,所以在基部通气最高,因此在吸气时肺部膨胀更多。由于肺循环中的灌注压相对较低,灌注在基部也最大。在疾病中,肺血管系统还通过确保肺部通气良好的区域接收大部分肺血流来使PaO 2最大化,这一过程称为V / Q匹配。这主要通过称为缺氧性肺血管收缩(HPV)的过程来实现。52与在体内所有其他血管床相比,肺循环在这方面是独特的,其在约8kPa(60mm Hg)的阈值下响应于缺氧而扩张。52在肺的通风不良的区域,所述前毛细血管肺动脉收缩响应于感测低肺泡PO 2(PAO 2)。这是一个补偿过程,尽管如此,一些脱氧血液仍可能留下通风不良的肺泡毛细血管单位。作为PaO 2和CaO 2之间的关系,通过与通风良好的单位的血液混合,无法补偿通气不良的肺泡毛细血管单位的脱氧血液不是线性的。这种生理现象往往得不到充分认识,因此值得一个理论上的工作实例(见专栏)。
调节V / Q匹配的研究较少的现象是缺氧支气管扩张。这种效果增加了肺部通风不良区域的通气。53
如果PaO 2下降,颈动脉体中的外周化学感受器会增加通气量以增加PaO 2。54这不会显着增加血液中的PO 2,而已经通风良好的单位,但会增加PO 2,通过增加这些单位的PAO 2,留下通风不良的肺泡单位。虽然对SaO 2和CaO 2的通气反应是线性的(图4),但颈动脉体感觉到PaO 2而不是CaO 2。这可以防止对贫血的过度通气,这对于增加CaO 2是无效的。外周化学感受器能够做到这一点,因为DO 2与颈动脉体的氧消耗的非常高的比率意味着颈动脉体中的组织PO 2继续反映PaO 2并且即使在贫血缺氧的情况下也不会下降。55 ,56
例
在氧疗之前,假设50%的肺流量通过低V / Q区域,并且来自该隔室的肺静脉氧合血红蛋白饱和度(SpvO 2)为80%(即刚好在混合的静脉SO 2之上)。另外50%通过匹配V / Q的区域,导致SpvO 2达到97%。最终的混合SpvO 2将是88.5%。
以下最大氧疗法,假定在流没有变化作为HPV,SpvO的释放的结果2从低V / Q间隔上升到85%和SpvO 2从匹配隔室上升到最大值的100%。得到的混合SpvO 2现在仅为92.5%。之所以发生这种情况,是因为除了溶解氧的最小贡献外,尽管PO 2增加,但完全饱和的血液不能使其氧含量增加到超饱和状态; 也就是说,PO 2与氧合血红蛋白饱和度/血氧含量之间的关系不是线性的。
Oxygen dissociation curve with Bohr effect. 2,3-DPG, 2,3-diphosphoglycerate; PO2, oxygen tension.
Erythropoiesis is controlled by a negative feedback system involving erythropoietin. By contrast with the carotid bodies, the peritubular cells in the kidney are well suited to sensing oxygen delivery as oxygen extraction is relatively high compared with oxygen delivery.57 ,58 Although oxygen delivery to the kidneys as a whole organ is high due to high renal blood flow, DO2 is reduced to the renal medulla as oxygen can pass from arterioles to the postcapillary venous system by shunt diffusion due to the parallel organisation of arterial and venous systems.42 Consequently, the peritubular cellular PO2 is low. It falls to even lower levels following reductions in DO2 either as a result of hypoxaemia or low haematocrit.
氧 - 血红蛋白解离曲线显示血红蛋白SaO 2和PaO 2之间的关系(图5和表10)。曲线的曲线形状具有两个特定的特征,用于保护组织缺氧。曲线的上部是平坦的,这意味着PaO 2的显着下降仍然与几乎完全的氧饱和度相容。其次,曲线的陡峭部分意味着尽管氧合血红蛋白饱和度迅速下降,但PO 2保持相对良好。尽管逐渐降低饱和度,但这种性质有利于向组织持续输送氧气。59
总二氧化碳解离曲线。HbCO 2,氨基甲酰血红蛋白; PCO 2二氧化碳张力。
响应于其他代谢因素调节血红蛋白的携氧能力,以提高氧气吸收和递送的效率。60该曲线右移,由于温度的升高,二氧化碳分压2和氢离子浓度(低pH)的增加或2,3-二磷酸甘油酸(DPG)。向右移动可增强氧气向组织的释放,并提高氧气的可用性,称为玻尔效应(图5)。
相反的情况适用于肺部,其中较低的二氧化碳水平有利于血红蛋白的氧负荷。因此,SaO 2无法准确预测PaO 2,反之亦然,但表10给出了近似等价物。
Chronic hypoxaemia increases 2,3-DPG in erythrocytes, shifting the dissociation curve to the right and therefore increasing oxygen delivery to the tissues. Levels of 2,3-DPG are reduced in stored blood reducing to zero after about 2 weeks. This may reduce oxygen delivery to the tissues but the magnitude of this effect is not thought to be clinically significant. Once transfused, levels of 2,3-DPG increase to about 50% normal after about 6 hours and back to normal within 48 hours.
Acutely, the cardiovascular effects of hypoxaemia will tend to counter the impact of lower CaO2 on DO2 by increasing cardiac output through increased heart rate and myocardial contractility and by decreasing afterload by reducing systemic vascular resistance.61 ,62 Anaemic hypoxia is sensed in the aortic body, presumably owing to lower perfusion relative to oxygen consumption. Consequently, the aortic body can act as a sensor of reduced oxygen delivery as a result of either low PO2 or low haematocrit (unlike the carotid body).55
At local tissue level, oxygen delivery can be adjusted to changes in local oxygen consumption. For example, exercising skeletal muscle receives a greater proportion of total cardiac output than resting skeletal muscle. This relates in part to hypoxaemia recruiting a larger proportion of the capillary bed by the relaxation of pericytes, and also through arteriolar vasodilation.63
Hypoxia may result from a number of different diseases discussed in section 8 of this guideline.
肺部肺泡毛细血管单位的血液中的缺氧缺氧可能是由肺泡缺氧或不完全气体交换引起的(见3.2节的定义)。这可能是由于吸入的氧分压降低,即高海拔,肺内分流,V / Q不匹配,肺泡通气不足或扩散损伤。
肺泡气体方程式使用以下公式计算肺泡中的氧气水平:
其中PAO 2和PACO 2代表氧气和二氧化碳的肺泡水平,RER是呼吸交换比率或二氧化碳产生与氧气消耗的比率和灵感PO 2(PIO 2)= FiO 2 ×(气压(100 kPa, 750毫米汞柱 - 水蒸气压(~6千帕,45毫米汞柱))。
考虑到这个等式,可以通过减少PIO 2或增加PACO 2来诱导肺泡缺氧。如果肺泡毛细血管单元的灌注程度相对不足(低V / Q比),PACO 2将由于间隙不足而上升,因此PAO 2将下降。这可能由于多种原因而发生,例如在呼吸衰竭的浅呼吸的非疲劳模式期间死区通气增加或晚期COPD中的肺功能异常。在导致全球通气不足的疾病中,例如呼吸肌无力,有效地肺的所有区域都具有低V / Q比率,这解释了与这些病症相关的高碳酸血症和低氧血症。
低V / Q病理生理学的极端形式发生在肺内和肺外分流中,其中根本不发生气体交换。肺内分流的一个例子是当肺段的气道被粘液阻塞时,产生灌注但不通气的肺组织区域,从而起到从右到左分流的作用。肺外分流的一个例子是在Eisenmenger综合征中伴有右向左分流的室间隔缺损。
在健康和静止时,PO 2与组织PO 2平衡,穿过肺泡毛细血管膜沿着毛细管长度的三分之一。随着该膜厚度的增加,如在纤维化肺病中,平衡可能需要更长时间,并且在毛细管末端的肺泡和血液之间可能存在氧梯度。当多个肺泡毛细血管单元受到影响时,其总体效果将导致肺泡 - 动脉(A-a)梯度增加。在运动期间,当毛细血管通过时间减少时,这会加剧。
贫血和一氧化碳中毒可能通过降低携氧能力导致“贫血缺氧”(参见第3.2节中的定义)。即使在没有低氧血症的情况下,低心输出量状态也会减少氧气输送。在这些情况下可能发生组织缺氧,这通常被称为“停滞缺氧”。“组织毒性缺氧”是由于无法在线粒体水平代谢氧气,可能是由于严重的败血症或某些类型的中毒。
高氧血症可由高氧血症和多发性血症引起。再次考虑上一节中的肺泡气体方程,高氧血症只能存在于高PIO 2或低PACO 2(由过度换气引起)的情况下。术语“高氧”在技术上可用于描述无高氧血症的多发性血症患者,但大多数临床医生仅使用该术语来描述PaO 2升高的情况。
Carbon dioxide is principally carried in the blood in three forms: carbon dioxide, bicarbonate and as a carbamino compound.64 In the normal physiological range of 4.6–6.1 kPa (34–46 mm Hg) the relationship between PaCO2 and carbon dioxide content can be considered linear (figure 6).
Effect of PaCO2 on ventilation with interaction of acidosis and hypoxaemia. PaCO2, arterial carbon dioxide tension; PCO2 carbon dioxide tension; PO2, oxygen tension.
PaCO2 is sensed at the peripheral54 and central chemoreceptors (in the medulla oblongata) by its effect on intracellular pH.65 Consequently, the regulation of PaCO2 is intimately related to pH homoeostasis (figure 7).
Example of oxygen alert card.
It is often not appreciated how V/Q matching relates to PaCO2. As discussed in section 5.2.1, alveolar capillary units with a low V/Q ratio have increased PACO2. Because of the high solubility and diffusibility of carbon dioxide, there is little A–a gradient for carbon dioxide at the end of the capillary, so blood leaving low V/Q alveolar capillary units has a high PCO2.
如上所述,低V / Q的区域通常通过HPV最小化。还认为高PCO 2可引起肺血管收缩,增加肺的同质性机制,使灌注与通气相匹配。66 ,67作为PCO之间的关系2溶解在血液和二氧化碳大约在生理范围内是线性的(不像氧),血液不会变得饱和与二氧化碳和因此高的肺静脉PCO 2从大V / Q区域可通过低肺静脉PCO 2部分平衡来自高V / Q区域。因此,通过增加整体肺泡通气,心肺系统能够预防高碳酸血症,尽管V / Q不匹配或分流,除非呼吸力学有限。
与氧气运输(玻尔效应)一样,PO 2和二氧化碳运输之间存在相互关系。这被称为Haldane效应。60脱氧血红蛋白比氧合血红蛋白具有更高的二氧化碳缓冲能力。这有利于全身静脉循环中的二氧化碳吸收和肺中的二氧化碳释放。
急性地,二氧化碳作为心脏上的拟交感神经药:它增加心率和每搏输出量,增加心输出量。它周围会引起血管舒张,降低全身血管阻力。在局部,二氧化碳充当血管扩张剂,从而将血流转移到具有高代谢需求的组织。由此产生的高碳酸血症的体征在7.2节中描述。
高碳酸血症的机制比低氧血症更简单,有四种可能的原因:68
吸入气体中二氧化碳浓度增加。
二氧化碳产量增加。
通气不足或通气不畅。
增加了外部死角。
COPD中的高碳酸血症(以及易患高碳酸血症性呼吸衰竭的其他病症)的机制将在6.3.1节中讨论。
这种医源性高碳酸血症的原因并不常见,但在从外部设备呼吸或通气时,任何意外发现为高碳酸血症的患者应首先排除这种原因。由再呼吸引起的高碳酸血症的严重程度受到PCO 2可以增加的速率(不超过0.4-0.8kPa / min,3-6mm Hg / min)的限制。
如果通过人工方式固定每分钟通气并且如果二氧化碳产生增加(例如,由于败血症或增加的呼吸功),则这可能仅引起高碳酸血症。
Low alveolar minute ventilation is by far the most common cause of hypercapnia. In clinical practice, COPD is the most common disease to cause hypercapnia; the problem is secondary to alveolar hypoventilation rather than a reduced minute ventilation per se. Patients adopt a rapid shallow pattern of breathing during an AECOPD with the result that the ratio of dead space to tidal volume is increased with more ventilation therefore being ‘wasted’. A rapid shallow pattern of breathing results in a bigger proportion of each breath being wasted because of the need to ventilate the anatomical dead space. Furthermore, during acute COPD exacerbations, V/Q mismatch may lead to an increase in physiological dead space, exacerbating the problem further. It is important to note that this commonly occurs in the context of an apparent overall increase in minute ventilation thus hypoventilation being a relative rather than absolute term. Adequate ventilation cannot be achieved since the respiratory muscle ‘pump’ is unable to overcome the load as a result of underlying respiratory mechanics. Alveolar hypoventilation due to a reduction in minute ventilation is seen following medullary respiratory centre depression by drugs, obstruction of a major airway or restriction of the lungs or chest wall or by respiratory muscle weakness, head injury, intracerebral haemorrhage or opioid narcosis.
Increased external dead space: This would be most common in patients breathing through artificial apparatus which has been incorrectly configured. Although alveolar hypoventilation is the most common cause of hypercapnia, it is important to consider the other potential causes, particularly when patients are receiving assisted ventilation and an artificial breathing circuit is used.
低通气化可能是生理性的 - 例如,在代谢性碱中毒的情况下。当呼吸肌无法使肺充分通气时会发生病理性通气不足,因为它们在病理上较弱或者它们不能克服异常的肺力学,例如在COPD恶化期间。由具有镇静特性或神经损伤的药物引起的呼吸驱动减少也会导致通气不足。
使用相同的生理学原理,但相反,过度换气由于任何原因将产生低碳酸血症。这可能发生在焦虑发作期间或生理过度通气期间的纯过度通气期间。
氧疗增加PAO 2,因此仅在肺泡毛细血管单元具有一些功能性通气时才有效。如果存在纯粹的分流(例如肺动静脉畸形),其中混合的静脉血不通过肺泡毛细血管单元,则氧疗是无效的。由于来自通气肺泡毛细血管单元的肺静脉血中溶解氧的增加,PaO 2仅有少量总体增加,这与血红蛋白携带的氧含量相比较小。尽管如此,有充分的证据表明呼吸氧气可以增加屏气时间。69-71一项研究发现,15名健康参与者的屏气时间从呼吸空气后56秒增加到呼吸4升鼻氧2分钟后92秒,另一项研究发现31名健康志愿者屏气时间增加从呼吸氧气32秒到呼吸氧气后61秒,29例慢性肺病患者的屏气时间为9秒,而呼吸氧气后29例患者的呼吸时间为22秒。在麻醉期间插管前使用相同的原理使患者预氧化,允许麻醉诱导和气管内导管通过之间更长的安全期呼吸暂停。
在通风不良的单元中(即,低V / Q比),PAO 2将是低的。增加FiO 2将增加PAO 2,因此增加PaO 2。低通气障碍可被视为完全由低V / Q单位组成的肺。
当由于肺泡毛细血管膜厚度增加而存在扩散限制时,例如在纤维化肺病中,增加PAO 2将通过增加浓度梯度来增加穿过肺泡毛细血管膜的扩散速率。
通过氧疗增加血浆中的溶解氧也可用于在一定程度上抵消低灌注的影响(停滞缺氧),并且在某些情况下(心源性休克)可能很重要,尽管效果仅是微不足道的。增加吸入氧气只能轻微减轻贫血缺氧的影响,但由于贫血患者的CaO 2低于正常血红蛋白患者,因此在这些情况下,溶液中携带的额外氧气的影响可能会变得更加重要。
组织氧合取决于向组织输送最佳或足够的氧气(DO 2)。该生理过程由各种组分组成,这些组分独立地和相互依赖地影响和确定DO 2并因此确定组织氧合作用。可以顺序考虑这些组件。
氧疗的生理学已在前一节中讨论过。然而,增加FiO 2仅是增加肺中氧摄取的一个组成部分。确保氧气输送到肺泡毛细血管床的其他关键操作包括:
保持令人满意的气道。
确保足够的肺泡通气。
逆转任何呼吸抑制剂,如麻醉剂。
Invasive ventilation or NIV where necessary.
Treating airflow obstruction by bronchodilation or sputum clearance techniques.
Optimising transfer factor (diffusion capacity).
Treatment of pulmonary oedema.
氧气主要通过血红蛋白携带在血液中,只有非常少量的氧气溶解在血液中。因此,足够的血红蛋白对CaO 2至关重要。最佳CaO 2的理想血红蛋白水平以及最佳DO 2长期以来一直是争论的主题。以前的做法有利于血红蛋白水平接近100 g / L(10 g / dL),提供足够的CaO 2以及降低血液粘度,以便在重症患者中更好地灌注血液。然而,加拿大研究人员在20世纪90年代后期的研究表明,70 g / L(7 g / dL)的血红蛋白水平与较高水平一样安全,并且可能在重症患者中产生较少的并发症。72然而,这项研究是使用非白细胞耗尽的血液进行的,并且可能通过使用白细胞耗尽的血液可以避免给予更多输血的组中的一些感染性并发症。因此,重症患者的最佳输血目标仍然是重症监护医学专家正在进行的讨论的主题。尽管不稳定或有症状的冠状动脉疾病患者的最佳血红蛋白问题尚未解决,但建议血红蛋白水平为100 g / L(10 g / dL)以获得足够的DO 2(见专栏)。
除了足够的CaO 2和PaO 2,氧气的输送取决于充足的含氧血液流量。心输出量又取决于足够的血液(循环)体积,足够的静脉回流以及足够和最佳的心肌功能。因此,为了避免组织缺氧,必须注意患者的体积状态和心脏功能的充分性,以及开始氧疗。在严重受惊的患者(例如,心源性休克,脓毒性休克)中,通常在适当的较高依赖性环境中指示侵入性监测和变力性/血管加压药治疗。一些研究表明,故意增加重症患者和高风险手术患者的氧气输送可减少器官衰竭,减少ICU停留时间,最重要的是,可提高死亡率。73-76然而,通过实现心脏指数的超常值或混合静脉血氧饱和度的正常值,有大量证据表明对发病率和死亡率没有有利影响。77-79
由于本指南涉及医疗环境中的紧急氧疗和氧疗,本节将重点介绍急性低氧血症的影响和风险。第8节将讨论与慢性低氧血症相关的长期疾病患者急性低氧血症的紧急治疗。在正常pH和温度下PaO 2和SaO 2之间的近似关系显示在表10和图5中(氧解离曲线)。表11总结了低氧血症的影响和风险。严重的低氧血症可能导致脑损伤和死亡。通常,低氧血症的许多生理作用是由低PaO 2介导的,不论含氧量如何。例如,即使在存在聚眼血症时总血氧含量正常,低氧血症仍将发挥生理作用,例如刺激通气。然而,低氧血症的风险通常由低组织PO 2介导,其可能由于低PaO 2和其他机制(例如严重贫血和低心输出量状态)而发生。这些问题可以在心肌缺血的病理生理学中得到说明,当心肌DO 2和氧消耗(V 2 O 2)之间存在不平衡时,这会产生心肌缺血。DO 2不仅依赖于PaO 2,还依赖于冠状动脉血流和血细胞比容。VO 2还将取决于心脏的中风工作。因此,鉴于其他变量,定义被认为是安全的PaO 2的下限是不可能的。低氧血症是指血液中PO 2异常低(见3.2节)。然而,不可能定义对所有患者都有危险的单一水平的低氧血症。慢性肺疾病有些患者可能习惯于与血氧饱和活2低至80%(PAO 2约6千帕或45毫米汞柱),而其他患者可能通过适度低氧血症受到伤害。已经表明,与饱和度保持> 90%的医学患者相比,持续饱和度<90%的医学患者的中期存活率受损。29
Recent observational data have shown a step-wise increase in mortality in hypoxaemic acute medical patients breathing air; the lowest mortality (3.7%) was found in patients with saturation ≥96% and this increased incrementally to mortality above 25% among patients with saturation <88%.19 However, much of this survival disadvantage may be due to the underlying disease which has caused the low oxygen level (eg, severe COPD or pneumonia) with the degree of hypoxaemia being a marker of disease severity. Furthermore, the mean and median oxygen saturation of patients aged >65 and the lower limit of the interquartile range (IQR) was about 2% lower than the saturation level of young adults so it is likely that much of the increase in mortality associated with modest hypoxaemia was related to the age of the patient. Therefore, the contribution of modest hypoxaemia to mortality rates is not known.
Mental functioning becomes impaired if the PaO2 falls rapidly to <6 kPa (45 mm Hg, SaO2<80%) and consciousness is lost at <4 kPa (30 mm Hg, SaO2<56%) in normal participants.80–83 Young participants tolerate acute hypoxaemia for longer than older participants in terms of ‘time of useful consciousness’.83 Safe levels of hypoxaemia in COPD have been discussed in detail in a review by Murphy et al.84 Many patients with COPD have a PaO2 of <5 kPa (37.5 mm Hg) corresponding to a SaO2 of <70% during an acute exacerbation.85 Furthermore, sudden hypoxaemia is more dangerous than hypoxaemia of gradual onset both in health and in disease. For example, millions of people live at altitudes above 3000 m despite an average PaO2 of about 7.3 kPa (55 mm Hg, saturation about 88%) and acclimatised climbers on Mount Everest can tolerate short-term exposure to an oxygen saturation of 54% or less with an estimated PaO2 of about 3.3 kPa (25 mm Hg).26–28 ,34 ,86 Campbell87 summarised this issue eloquently in 1967 when he said “Better a year at a PaO2 of 50 mm Hg (6.7 kPa) than an hour at a PaO2 of 20 mm Hg (2.7 kPa).”
当PaO 2降至40 mm Hg(5.3 kPa)以下时尿液流量和肾功能突然下降,相当于氧饱和度达到~74%,88据报道,与氧气水平相关的呼吸衰竭患者缺氧性肝炎4.5 kPa或34 mm Hg,而心脏病患者的缺氧性肝炎主要是由于肝血流减少(停滞缺氧)和血氧水平较高。89 ,90在飞行中与平均血氧饱和度COPD患者的研究2在海平面96%,显示出在商业客机下降到90%,在飞行和进一步下跌至平均血氧饱和度2在飞机过道中行走时占87%。这些患者在这些低氧血症发作期间没有症状。91一项针对84名健康航空公司乘客的研究发现,平均SaO 2从地面的97%下降到巡航高度的93%(1SD 85-98%)。92一项针对健康航空公司机组人员的研究显示,乘务员的SaO 2降至最低点80%至93%(平均88.6%),不会引起呼吸困难或任何其他症状。93
没有任何随机证据,指南制作小组已经建议,没有任何症状(约85%饱和度)的健康人所耐受的饱和度应被视为低氧血症的安全下限。但是,可能需要考虑其他合并症,专家意见建议对于重病患者,应将SaO 2维持在90%以上。29-32因此,本指南推荐了目标SaO 2(和SpO 2))大多数低氧血症患者≥94%,以确保大部分时间的实际氧气水平保持在90%以上,安全范围为4%,以允许氧饱和度水平,记录和血氧计误差的变化。血氧饱和度的准确性和缺陷在7.1.2节中讨论。
本节将从理论上考虑各种疾病中氧疗的具体目标,实际上将在第8和第9节中考虑。一些患者 - 尤其是老年人或患有慢性肺病的患者 - 临床稳定时应该具有低于94%的SaO 2和氧气应该如果患者临床稳定,不仅仅是为了将SaO 2维持在94%以上。在评估病人时,SaO 2水平只是应该监测的几个生理变量之一。许多患者突然急性疾病,例如手术后肺栓塞将在生理变量的突然改变由“轨道和触发”系统所评估,如改性预警评分(MEWS)系统94 ,95或英国新闻。96名此类患者可仅具有小下降血氧饱和2由于生理补偿机制,例如增加的通风。因此,即使在推荐的目标范围内,医疗保健专业人员也需要警惕SaO 2的跌倒。由于SaO 2的正常范围很宽,以及关于轻微低氧血症可能的生理后果的不确定性,2008年指南组中关于理想目标范围的争论比指南的任何其他方面更多。如果是SaO 2应该略低于94%,关键问题是识别和治疗跌倒的原因(例如,肺栓塞),而不仅仅是纠正低氧血症,这在本级别本身可能不是危险的。然而,医疗保健工作者可能无法对异常的低氧血症做出适当的反应。经过多次辩论后得出结论,该指南将建议所有成年患者的目标范围为94-98%。这反映了健康成人中SaO 2的近似正常范围,如3.1节所述。然而,SaO 2持续下降> 3%,即使在正常范围内,也可能是急性疾病的指标,应该要求对患者进行临床评估,而少数患者(特别是年龄> 70岁的患者)可能患有血氧饱和度即使临床稳定,2例<94%。
急性低氧血症被认为对低于PaO 2约6 kPa(45 mm Hg)或SaO 2约80%的健康参与者是危险的,因为精神受损和组织缺氧风险,但患有急性疾病或慢性器官疾病或缺血的患者可能存在高于此水平的风险,重症监护指南建议旨在达到> 90%的饱和度。
生理“追踪和触发”系统(如NEWS 96)的变化可能发生在急性疾病中,无论是变化还是SaO 2水平只有很小的变化。
Critical illness may present initially with only a small fall in SaO2 level because of compensating mechanisms.
The upper end of the recommended range in this guideline (98%) is the upper limit of SaO2 in healthy adults.
The lower end of the suggested target saturation range (94%) is close to the lower end of the normal range and ensures that the SaO2 remains above 90% even if it falls slightly below the target range.
如本指南所述,补充氧疗最常用于纠正低氧血症。然而,在某些情况下,可以给予非低氧血症患者补充氧气以实现高氧血症。这需要区别于高压氧疗法(高于大气压的氧气疗法),这超出了本指南的范围。
一氧化碳和氰化物中毒(见8.10.7节)
自发性气胸(见第8.11.6节)
一些术后并发症(见8.15.3节)
集群头痛(见8.13.7节)
大多数CPR指南和危重病患者的护理建议在复苏的初始阶段使用最高可行氧浓度。尽管这些建议不是以证据为基础的,但在这些紧急情况下不可能使用不同水平的氧疗进行对照试验,并且对于循环衰竭和呼吸衰竭的重症患者来说,最大限度地提供氧气似乎是直观的。然而,已经进行了呼吸室内空气或氧气的新生儿复苏的随机试验,并且Cochrane评价的意外结果是当使用室内空气时存活率更好。97这一令人惊讶的发现不能外推给成年患者,但它确实强调了临床试验的必要性,即使在人们可能直观地认为氧气有益的领域也是如此。此外,有理论证据表明,心脏骤停后恢复自发循环的患者可以通过<100%吸入氧气更安全地进行治疗。98 ,99最近的观察性研究表明从hyperoxaemia可能产生的有害结果在心肺复苏的幸存者在第8.10.1进行了讨论。
已经表明,在危重病人以及高风险手术患者中增加向组织的氧输送的早期干预减少了器官衰竭,减少了ICU停留时间,并且最重要的是,提高了存活率。73-76氧气输送增加部分涉及氧气治疗,但这些研究并未显示出针对超生理氧气输送的任何益处。有证据表明,高氧血症可能与ICU患者的死亡率增加有关,这将在8.10.2节中讨论。
据报道,氧疗法治疗已确定的伤口和治疗伤口败血症的益处是有争议的。高压氧降低了慢性糖尿病足溃疡患者的截肢风险,并可能提高1年内愈合的机会,但Cochrane评价员对现有研究的规模和质量表示担忧,并建议进一步试验。100目前尚不清楚传统的氧疗是否对伤口愈合有任何影响。101
第8.15.3节讨论了氧气预防术后伤口感染的潜在益处。
通过缓解呼吸困难和呼吸功,氧疗可以减少二氧化碳的产生,从而抵消PaO 2的一些潜在增加,否则可能由于6.3.1节中描述的机制而发生。然而,没有支持使用氧气进行该适应症的对照试验。
这些总结在表11和Downs 102以及其他来源的评论中。103-107以下段落将总结补充氧疗和高氧血症的生理学和病理生理学。
The most significant effect of high-concentration oxygen therapy on the respiratory system is hypercapnic respiratory failure in a population of vulnerable patients as described more fully in section 8.12. This does not occur in the absence of significant pulmonary disease or musculoskeletal disease affecting the thorax, and it can occur while the PaO2 is still within the normal range or slightly below normal, especially in patients with exacerbated COPD for whom the baseline oxygen saturation level may be well below the lower limit of normal.
几十年来人们已经说过,“高氧血症”会导致患有内源性肺病(如COPD)的患者呼吸运动减少导致高碳酸血症性呼吸衰竭,而且从20世纪60年代到现在,很多(如果不是大多数)医学教科书都提到了'当给予AECOPD患者高浓度氧气时,缺氧驱动器是导致高碳酸血症和酸中毒的主要原因。这种说法通常归功于Campbell在20世纪60年代倡导控制氧疗的概念。然而,坎贝尔87被广泛误导。他在1967年实际上所说的内容如下:“通常将这些患者的PaCO 2升高归因于去除通气的缺氧驱动但我同样对疼痛和同事产生怀疑。108这是整个故事; 肺循环的变化也可能是重要的。”大部分但不是全部随后的研究中48 ,49 ,108-113显示,坎贝尔在这个假设是正确的,如第4.2节中讨论。AECOPD中高碳酸血症的另一个奇怪特征是它不是普遍的。87名有些COPD患者容易出现呼吸衰竭的反复发作和其他人可能永远无法从这一并发症困扰。即使在患有慢性高碳酸血症的COPD患者中,并非所有患者在急性发作期间都会出现增加的二氧化碳水平(和酸中毒)。PaCO的观察进一步混淆了作为高碳酸血症原因的“缺乏缺氧驱动”的理论随着PaO 2升高超过13 kPa(100 mm Hg),2继续上升,这对减少通气几乎没有影响,大多数COPD恶化期间患有呼吸性酸中毒的患者PaO 2高于10 kPa,相当于高于约93%的饱和度。43因此,虽然在通风少量减少可以是在COPD氧气治疗期间二氧化碳水平上升的一个因素,主要因素是第V / Q匹配的恶化。增加FiO 2的附加效果将与肺不张有关,并且可能由于粘度增加而恶化气流阻塞。在肺内疾病很少但呼吸肌无力的情况下,缺氧性呼吸驱动的丧失将是高碳酸血症发生的更大因素。然而,即使在非患病的肺中,HPV仍然是V / Q匹配的重要调节剂。
虽然氧诱导的高碳酸血症的机制仍然存在争议,但可能至少有六种机制对此负责。这些按可能的顺序排列如下:
V / Q不匹配,
通气驱动,
Haldane效应,
吸收性肺不张
与空气相比,氧气密度更高,
如果通过面罩使用低氧气流速,则可能发生再呼吸。
在呼吸空气期间,通风不良的肺泡毛细血管单元将缺氧,因此由于HPV导致灌注不良。如果施用高浓度氧气,PAO 2将上升,从而逆转HPV并增加血液流向该单位。然而,虽然装置中的氧气增加,但是它仍然通风不良,具有高PACO 2,因此高肺静脉PCO 2。随着越来越多的血液通过这些单位,PaCO 2将会上升。通常,当没有明显的肺部疾病或胸部肌肉骨骼疾病时,呼吸系统能够通过增加整体通气来补偿这些变化,从而降低PaCO 2。然而,如果呼吸力学导致通气量增加,PaCO 2将上升。一些作者报道,当给予补充氧气时,这种机制比减少通气驱动产生高碳酸血症更重要,但这仍然是呼吸生理学的一个有争议的领域。48 ,49 ,108-113
低氧血症会增加通气量,因此低氧血症的缓解会导致通气减少。随之而来的PaCO 2上升与通气量的减少成反比,使得假设二氧化碳产量恒定,肺泡通气减半将导致PaCO 2加倍。如图4所示,PaO 2高于8 kPa(60 mm Hg)的任何增加都不会显着降低通气量,增加高于13 kPa(100 mm Hg)对通气几乎没有影响,因为颈动脉窦放电在很大程度上减弱了13以上千帕。因此,该机制仅对于解释当PaO 2时PaCO 2的增加是重要的升至13 kPa,但此后不再增加。这种现象也见于正常人。一些临床研究表明,“缺氧驱动”对PaCO 2升高的贡献很小,临床上可见COPD患者使用高浓度氧气,但最近的一项研究支持了这一机制。48 ,49 ,108-113
增加FiO 2的第三个作用是通过Haldane效应60降低血红蛋白的二氧化碳缓冲能力(见5.3.2节)。
第四种效应,即吸收性肺不张,被认为是由于肺泡吸收氧气而导致高PAO 2超出阻塞气道。这可能发生在FiO 2低至30-50%并且将导致分流(增加的V / Q不匹配)。102
Johnson 等[ 114]表明,与呼吸空气相比,呼吸纯氧的患者FEV 1降低。他们得出结论,这种影响可能与氧气相对于空气的密度和粘度略有增加有关。这会增加呼吸功,这可能导致疲惫的患者出现高碳酸血症。
这个问题在第10节和Jensen 等人的论文中讨论过。115
在高浓度氧气治疗后出现失代偿性高碳酸血症呼吸衰竭的患者,如果突然停用氧气以试图纠正过量氧疗的影响,则面临进一步显着的低氧血症反弹的危险。116 ,117
可以使用肺泡气体方程来解释反弹性低氧血症,并且鉴于其重要性,最好用工作实例(方框)来说明。出于简化的目的,该实施例做出若干假设,例如恒定的呼吸交换比和阶段1和3之间的A-a梯度。它还假设通风保持不变。虽然当PaO 2在去除氧气时降至3.4kPa,通风将上升,根据定义,由于首先出现高碳酸血症呼吸衰竭的相同原因,它不能充分升高以满足清除二氧化碳储存的需要。反弹性低氧血症是一种主要风险,可能导致死亡。因此,本指南将建议逐步降低氧疗,同时持续监测饱和度。
好的做法点
突然停止补充氧疗可引起反应性低氧血症,PO 2迅速下降至低于补充氧疗开始前的张力。
例如:反弹性低氧血症
第1阶段:考虑COPD恶化的患者,其ABG如下:PaO 2 6.5 kPa; PaCO 2 7.5 kPa呼吸室内空气。假设呼吸交换率为0.8,由肺泡气体方程式(5.2.1)计算的PAO 2为11.6,A-a梯度为5.1kPa。
阶段2:通过储液袋面罩给予最大氧气,他的血气变为:PaO 2 32 kPa; PaCO 2 10 kPa。由于二氧化碳的高溶解度,二氧化碳的总体储存量将增加。
阶段3:如果突然停止氧疗,PACO 2和PaCO 2最初将保持高水平,因为二氧化碳储存量高,因此PAO 2将比氧气治疗前的最初降至8.5 kPa。假设室内空气呼吸的A-a氧气梯度保持在5.1kPa,那么计算的PaO 2将变为3.4kPa。
在循环的影响和hyperoxaemia的潜在危害进行了总结,汤姆森等人105,其中提出了强烈的情况下,更多的临床试验的社论。高氧血症引起冠状动脉和脑血管收缩,如果血细胞比容足够低,理论上可能由于DO 2的总体减少而导致反常的组织缺氧。有报告称,对于轻度至中度严重中风的非低氧血症患者,或者对于心肌梗塞的非低氧血症患者,如第8.13.1和8.13.2节所述,可能会对氧气给药造成伤害。汤姆森等人105已经建议,应该“小心地”规定,给药和监测氧气,以“实现最佳组织氧合”,而不是最大限度的氧合作用。这一观点是由其他作者如布莱恩和詹金森118在20世纪80年代提出的,但标准医学实践在2008年第一版本指南发布之前没有注意到这一建议。因为没有公布的数据表明有益在大多数医疗条件下,由于高氧血症,并且由于理论上的风险,最佳管理应针对生理氧合作用。第8节讨论了在特定情况下有证据的氧疗目标。
除了高氧血症的潜在有害生理影响之外,由活性氧(ROS)介导的毒性作用具有潜在风险。118在过氧化氢和超氧化物形式的高组织PO 2存在下产生过量的ROS ,引起氧化应激和自由基损伤。119在生理水平,ROS充当信号分子,但在较高水平,它们具有细胞毒性,特别是被引发的中性粒细胞作为宿主防御机制释放。认为ROS是通气性高氧早产儿120和心肌梗塞后再灌注损伤中支气管肺发育不良的原因。121自19世纪以来,人们就知道在动物模型中长时间暴露于高浓度的氧气会导致弥漫性肺泡损伤,出血,肺泡萎陷,炎性细胞浸润,坏死,细胞凋亡以及肺内皮和肺上皮损伤。在一个大气压下暴露于73%氧气4天后,在大鼠模型中死亡。122 Griffith 等[ 123]在1986年证实,正常人肺受到30-50%氧气呼吸45小时,白蛋白渗漏到支气管肺泡灌洗液和其他肺损伤标志物中。123
之前认为高FiO 2具有保护作用,可为患者提供安全保障。然而,Downs 102和Beasley 等人106认为,通过预防性使用高浓度氧疗,实际上可能会使不稳定的患者处于危险之中。107 ,124在生理恶化,患者给予高浓度氧气疗法将具有正常或高脉冲血氧计读数在氧分压掩蔽逐渐下降2 /氧合指数2比,因此不提醒工作人员到即将发生的劣化,需要机械支撑。参考文献中显示了一个有效的例子。106此外,在低FiO 2下生理上恶化的患者将通过脉搏血氧仪早期检测到并且可以在转移到ICU时使FiO 2增加,而已经接受高FiO 2的患者将减缓更慢但是当血氧计最终检测到去饱和时,治疗选择会更少,因为进一步增加FiO 2几乎没有效果。88 ,92 ,107
氧是已知的危害患者百草枯中毒125 ,126和氧potentiates博莱霉素肺损伤,并且可以增强从酸抽吸肺损伤。127-129有关这些条件的更多细节见8.13.4节。
生理风险
更糟糕的V / Q不匹配。
吸收性肺不张。
冠状动脉和脑血管收缩。
心输出量减少。
氧自由基造成的伤害。
全身血管阻力增加。
临床风险
恶化的高碳酸血症呼吸衰竭。
延迟识别临床恶化。
轻度至中度卒中可能导致更差的预后。
先前博来霉素肺损伤或百草枯中毒或酸吸入患者的特殊风险。
正常血氧饱和度的急性冠状动脉疾病的未知风险 - 收益平衡。
与心脏骤停幸存者和ICU患者死亡风险增加有关。
不受控制的补充氧疗可能对有高碳酸血症呼吸衰竭风险的患者有害,特别是如果PaO 2升高到10 kPa以上。
高浓度氧疗法产生高氧血症(高于正常氧饱和度)并且与一些患者组(例如,轻度和中度中风患者,心脏骤停幸存者和ICU患者的死亡风险增加相关;见第8节)。
高碳酸血症和呼吸性酸中毒是密不可分的,最好一起考虑。如果高碳酸血症发展缓慢(持续数天),患者将获得肾脏补偿(碳酸氢盐的保留),并且在大多数此类病例中不会发生酸中毒。然而,血液二氧化碳水平的急剧升高会产生呼吸性酸中毒和高碳酸血症的症状。PCO 2升高的一些后果是由此导致的酸中毒的结果。有时候PCO的效果会增加2在特定的器官系统上,酸中毒的相反作用是对立的。二氧化碳是血管扩张剂,患有高碳酸血症的患者可能会出现外周静脉扩张和边界脉冲冲洗。颅内血管扩张可能引起头痛。高浓度的二氧化碳具有催眠作用,患有高碳酸血症的患者可能从困倦到混淆到昏迷。84 ,130-134的链接已显示出不适当的高血氧水平,由于高浓度氧气的使用和严重呼吸性酸中毒的急性与慢性阻塞性肺病机械通气死亡或要求的风险增加发展之间。43 ,46 ,135然而,呼吸性酸中毒的问题并不仅限于COPD患者。任何原因导致的呼吸衰竭都会导致高碳酸血症。例如阿片类药物过量,通气不足的肥胖和影响呼吸肌肉的神经肌肉疾病。最近的研究表明,OHS患者以及肺炎患者和哮喘急性发作患者的二氧化碳水平升高,其中高氧血症和高碳酸血症之间的联系以前未被发现。47 ,136 ,137
对大学医院4866名患者的血气进行的审计表明,高碳酸血症比来自外科病房,手术HDU,剧院和ICU以及医疗病房和医疗HDU的血气样本中的低氧血症更常见,其中许多高碳酸血症患者有呼吸性酸中毒。42此外,在急诊室530个血液气体试样瑞士审计表明,患者在最低pH三分位数更经常需要入院到ICU(28%比在第一三分位数为12%,P <0.001)和院内具有较高的死亡率(14%vs 5%,p = 0.003)。138高碳酸血症入院独立与入住ICU的风险增加,并在这项研究增加了30天死亡率。
神经系统
二氧化碳直接或作为酸中毒的结果发挥其作用。高碳酸血症会增加脑血流量,从而可能影响脑脊液压力。它是影响细胞内pH的主要因素,对细胞代谢有重要影响。它发挥类似于一氧化二氮的惰性气体麻醉作用。它影响神经元的兴奋性,特别是在网状激活系统中。当PaCO 2升至12-16 kPa(90-120 mm Hg)以上时,二氧化碳可诱发麻醉。130
肺循环
升高的PACO 2引起肺循环中的血管收缩,尽管其效果不如低氧血症。139在健康参与者中,7 kPa(52 mm Hg)的呼气末PCO 2使肺血管阻力增加32%,随着心输出量的增加,平均肺动脉压力增加60%。140 pH的变化被认为是导致二氧化碳介导的肺血管系统变化的主要因素。141 ,142因此,与HPV,在PACO变化2的帮助以匹配灌注通风。
呼吸系统
如第5.2.1节所述,升高的二氧化碳水平可能会加剧低氧血症及其影响,因为如果氮浓度保持不变,肺泡气体中的二氧化碳浓度会降低氧气浓度。此外,PaCO 2的增加使氧解离曲线向右移动。
心血管系统
通常,高碳酸血症和酸中毒对心肌细胞和血管平滑肌细胞具有直接抑制作用。143个这些现象是由于在引起所述凸起二氧化碳分压的儿茶酚胺的增加通常不是2。因此,二氧化碳对心血管系统的总体影响是不可预测的。在人工通气的儿童中,二氧化碳的增加会增加心输出量并降低总外周阻力并且血压趋于升高。144尽管二氧化碳的增加会降低心率,但由于儿茶酚胺刺激的作用超过对心脏的抑制作用,因此心动过速更常见。已经报道了心律失常,但在正常参与者中很少有临床意义。二氧化碳是一种全身性血管扩张剂。
肾脏
在存在高于约65mm Hg(8.7kPa)的PaCO 2水平时,肾血流量和肾小球滤过率突然降低。88 ,145
血液电解质水平
如果酸中毒严重且持续,伴随高碳酸血症的酸中毒可能导致钾升高。
内分泌系统
高碳酸血症可增加内源性肾上腺素和去甲肾上腺素的血浆水平。
高碳酸血症的临床症状由上述生理变化产生,并在7.2.1节中详细描述。
酸中毒的主要影响是严重酸中毒(pH,7.0或[H +] 100 nmol / L)引起定向障碍和后来的昏迷。然而,如上所述,pH的影响与低氧血症和高碳酸血症密不可分。由于酸中毒,低氧血症和高碳酸血症对个体患者不同靶器官的相反影响以及所有三种成分紊乱可能同时发生的事实,很难预测酸中毒本身的影响。个别病人。此外,组织缺氧会加剧酸中毒。其后果将取决于三个变量的相互作用,并与共病疾病状态的影响相结合。众所周知,在患有COPD的患者中,急性恶化期间的pH <7.30或[H + ]> 50nmol / L与更差的预后相关。43
氧疗通常被定义为氧浓度高于环境空气中的氧气。通常用于治疗或预防低氧血症,从而防止组织缺氧,这可能导致组织损伤甚至细胞死亡。临床医生必须记住,补充氧气可以改善氧合作用,但它不能治疗低氧血症的根本原因,必须作为紧急事项对其进行诊断和治疗。
在一些情况下,例如一氧化碳中毒或氰化物中毒或丛集性头痛,氧疗法用于实现高氧血症。随机研究的证据表明,与非低氧血症的COPD患者在运动后呼吸困难或患有晚期癌症的非低氧血症患者相比,氧气不能缓解呼吸困难。146-150在组织水平,线粒体活性需要氧气用于有氧ATP合成细胞活动。海平面干燥空气的PaO 2为21.2 kPa(159 mm Hg),但在线粒体中,PO 2根据组织类型和局部代谢活动,其在0.5-3.0kPa(4-22mm Hg)的范围内。这种从大气到线粒体的梯度称为氧气级联。该级联中有许多因素影响最终的线粒体PO 2,包括肺泡气体交换,血液中的氧运输和组织灌注。在病理条件下,该级联中一步的任何变化都可能导致线粒体水平的缺氧。因此,虽然不一定解决组织缺氧的根本原因,但增加FiO 2氧疗是避免低氧血症患者缺氧组织损伤的最简单,最快捷的方法。除氧疗外,通常还需要采取其他措施来改善向组织输送氧气(见5.6节)。
许多疾病状态导致低氧血症,并且呼吸困难患者的标准做法是用氧气治疗(参见4.3节)。然而,几乎没有对照试验比较不同水平的吸入氧气对任何导致低氧血症的常见疾病的患者。还必须记住,氧疗只是可用于增加危重病人组织氧输送的几种策略之一(见5.6节)。在许多临床情况下,应用氧疗而没有特定的终点。许多研究表明,高氧血症可能具有有害的生理和临床效果(见6.3节),尽管这种效应在COPD以外的病症中没有广泛报道。然而,高氧血症可能存在潜在的伤害,应遵循所有药物处方中的良好医疗实践。鉴于一些作者最近提出的建议,高氧血症可能与ICU患者和心脏骤停幸存者的风险增加有关,这一点尤其重要,尽管这一观点受到其他作者的质疑。151-156由于线粒体水平的实际PO 2变化很大且依赖于除PaO 2以外的许多变量,因此通常很难设定PaO 2的最低水平,低于该水平将发生确定的细胞损伤或高于该水平的宿主是安全免受缺氧细胞损伤的影响。此外,临床上不可能监测线粒体PO 2,并且唯一临床可用的线粒体缺氧替代物是乳酸产生。虽然血液乳酸水平是有用的并且可能表明组织低氧血症,但它是晚期标记物因此是不敏感的工具。因此,为“理想”血气水平设定的目标基于任意目标。
由于正常动脉氧水平随年龄自然下降,有人建议理想目标PaO 2可通过以下等式确定:理想PaO 2 = 13.3 kPa-0.04×年龄(以年为单位)或100 mm Hg- 0.3×年龄(以年为单位)。157就床边测量的氧饱和度而言,在大多数情况下,这将转化为94-98%的SaO 2。该策略避免了几乎所有患者的组织缺氧,并且还避免了高氧血症的潜在有害影响。因此,标准做法应该是将氧气规定为特定饱和度(或PaO 2)而不是FiO 2。显然,需要考虑对氧气敏感的二氧化碳保留的患者,并且这些患者可能需要设定较低的目标(通常为88-92%),以在实现理想和安全的SaO 2 / 之间取得平衡。PaO 2和二氧化碳保留。有一项随机对照试验,对于加重COPD的患者,目标范围为88-92%。51该试验得到了五十年的生理学和观察性研究的支持,这些研究将在8.12节中进行综述。具体的疾病状态将在第8节中讨论。患有中度至重度低氧血症的患者通常是呼吸困难并且呼吸频率增加。除了导致身体疲劳外,这也增加了呼吸功,因此增加了氧气消耗和二氧化碳产生。在这些情况下,氧疗可以减少呼吸功,从而减少二氧化碳的产生。因此,理论上氧疗应能改善低氧血症患者的呼吸困难。然而,尽管医生和患者普遍认为氧气可以缓解呼吸困难,在涉及气喘但非低氧血症的患者的临床试验中发现了很少的益处效应证据。例如,所有已发表的针对患有呼吸困难的COPD患者的短爆发氧疗法的盲法研究的一项荟萃分析报告了适度和异质性益处,另一项荟萃分析未能证实任何临床益处。146 ,158
对于患有任何原因的晚期疾病的患者,在2004年对氧气和气流进行系统评价以缓解呼吸困难,仅发现低级科学证据表明氧气和气流改善了一些休息时晚期疾病患者的呼吸困难,几乎所有这些参与者是低氧血症并且已经使用氧疗法。159 2010年发表的一项研究报告称,对于PaO 2 > 55 mm Hg(7.3 kPa)的患者,鼻导管输送的空气中的氧气对缓解与生命限制性疾病相关的难治性呼吸困难没有额外的症状益处。两个研究组的呼吸急促下降,与提供医用气体暂时相关。150
证据陈述
没有随机试验比较没有高碳酸血症呼吸衰竭风险的患者的不同氧饱和度水平。专家意见(基于生理学和观察性研究)建议维持这些患者的正常或接近正常的氧饱和度为94-98%(证据级别4)。
患有高碳酸血症风险的COPD患者的目标饱和度为88-92%(证据水平1+)。
根据从观察性研究推断的专家意见(证据级别4),具有高碳酸血症的其他风险因素(例如,病态肥胖,胸壁畸形或神经肌肉疾病)的患者的目标饱和度为88-92%。
在急性疾病中达到理想氧饱和度范围的建议(另见图1-2)
A1:本指南建议除了有高碳酸血症呼吸衰竭风险的患者(D级)外,所有急性病患者的氧饱和度均达到正常或接近正常水平。
A2:没有高碳酸血症呼吸衰竭风险的急性病患者的推荐目标饱和度范围是94-98%(D级)。
A3:对于已知COPD或其他已知的高碳酸血症性呼吸衰竭危险因素(例如,病态肥胖,CF,胸壁畸形或神经肌肉疾病或与支气管扩张相关的固定气流阻塞)的大多数患者,目标饱和度范围为88-92%。建议等待血气结果可用(COPD为A级,其他条件为D级)。
A4:大多数非低氧血症无呼吸患者不会从氧疗中受益,但患者在目标饱和度范围内的氧饱和度突然降低≥3%应该能够更快地评估患者(和血氧计信号),因为这可能是急性疾病的第一个证据(D级)。
患者的适当定位可以最大化V / Q匹配。在健康的自我通气成人肺中,V / Q匹配从非依赖性区域改善为依赖性区域。在肺病中,存在这种模式的破坏,并且在这些情况下,适当的定位可能有利于优化V / Q匹配,因此改善气体交换,氧合和二氧化碳清除。由于这些原因,呼吸困难的患者通常喜欢坐直或接近直立,只要他们能够这样做。无论参与者的位置如何,都保持依赖性和V / Q匹配之间的关系。然后,生理学可转移到交替的侧卧位; 例如,在左侧躺着依赖肺(左)将具有更好的V / Q匹配。这在存在不对称肺病理学时是重要的,因为“良好肺下降”原则将使V / Q匹配最大化。许多不适的患者在半卧位和仰卧位进行护理。由于隔膜和胸壁阻碍了依赖性肺的扩张,这些位置不利于V / Q匹配,如在直立和全侧躺卧位置。即使在健康的参与者PO2在仰卧位置比在直立位置低0.7kPa(5mmHg)。20类似地,患者的右侧偏瘫和伴随的胸部疾病10%是在左侧卧位更低氧血症。160如果存在病理性肺病并因此已经存在显着的V / Q不匹配,则可能进一步损害气体交换。这在一篇综述中讨论了位置对急性卒中血氧饱和度的影响。161患有无呼吸道合并症的急性卒中患者可以采用他们认为最舒适的任何身体姿势,而呼吸系统受损的患者应尽可能直立,避免慵懒或仰卧位以优化氧合作用。161半卧位/仰卧位通常用于救护车。此外,为了安全起见,患者使用腹部和胸部束缚将其手臂绑在担架上。虽然缺乏关于此的具体数据,但生理学原理表明使用这种定位和约束会损害呼吸肌功能和气体交换。最后,有一些罕见的肝病,心脏分流术或肺纤维化患者有“platypnoea和orthodeoxia”,这意味着他们在直立位置更缺氧。162其他患有脊柱侧凸或瘫痪的膈肌的患者可能会对“良好的肺部向上”感觉更舒服。应允许这些患者选择呼吸最舒适的位置。
证据陈述
来自许多队列研究的证据表明,在健康参与者和急性疾病中,仰卧位氧合作用减少,但没有对照试验显示特定身体位置的益处(证据等级4)
建议
A5:由于仰卧位氧合作用减少,理想情况下应该让完全清醒的低氧血症患者保持最直立的姿势(或患者最舒适的姿势),除非有充分的理由使患者固定不动(例如,骨骼或脊髓损伤)(D级)。
检查危重病人的临床医生应该记住急诊医学的“ABC”。在重症患者的情况下,可能需要在获得详细病史之前和可以进行全面体检之前确保气道并使患者复苏。此外,重要的是要记住补充氧气可以改善氧合作用,但它不会影响低氧血症的根本原因,低氧血症必须作为紧急事项进行诊断和治疗。
在评估病人时,SpO 2水平只是应该监测的几个生理变量之一。许多患者突发急性疾病如术后肺栓塞将所评定的监测和预警系统系统在生理“跟踪和触发”变量突然改变94 ,95 ,163和皇家医师学院开发的消息。96名此类患者可仅具有小下降血氧饱和度2由于生理补偿机制,例如增加的通风。因此,即使在推荐的目标范围内,临床医生也需要警惕SpO 2的跌倒。
虽然强烈建议使用“跟踪和触发”系统,但指南组对于有高碳酸血症呼吸衰竭风险的患者有一些保留意见,特别是2012版Royal College of Physicians NEWS,因为没有选择设定氧饱和度的目标范围。164 ,165有高碳酸血症呼吸衰竭风险的患者,如本指南所建议的,在88-92%的目标范围内,将获得2-3个EWS点,并可能促使护理人员增加吸入氧气水平以达到“正常”氧合作用(> 96%)并使患者处于危险之中。指南小组建议使用2017年更新的NEWS图表,该图表允许对有高碳酸血症呼吸衰竭风险的患者的饱和度评分进行适当调整。患者应在低于目标范围的饱和度下评分EWS点,或者在呼吸氧气时显着高于目标范围。2017年NEWS图表将为患有高碳酸血症风险的患者提供特殊的血氧测定部分。
证据陈述
没有针对急性不适患者的不同评估方法的对照试验。关于临床评估的建议基于专家意见和结果的回顾性研究(证据级别4)。
建议
B1:训练有素的临床医生应通过测量呼吸频率,脉搏率,血压和体温,评估循环血容量和贫血来评估所有急性病患者。如果患者被认为患有重大危及生命的疾病,应尽早寻求重症监护专家或其他学科的专家协助,临床医生应准备在必要时呼吁提供帮助,包括在院前护理中呼叫999救护车或致电复苏团队或ICU外展团队进行医院护理(D级)。
低氧血症的传统临床评估包括临床检查皮肤和颊粘膜,以确定是否存在中心紫绀。这是一项困难的临床技能,尤其是在光线不足的情况下。由于存在贫血或红细胞增多症,低氧血症的临床评估变得更加不可靠。在正常SaO 2存在的情况下,一些患者可能由于外周循环不良而出现外周紫绀。一些研究表明,低氧血症通常不被紧急医疗服务提供者所认可,特别是如果患者不抱怨呼吸窘迫。166-1682005年文献的系统评价报道,大多数低氧血症患者至少有一种生命体征异常,但与脉搏血氧测定相比,皮肤颜色是低氧血症的不良指标。39由于这些原因,建议临床医生不要依赖“紫绀”的视觉评估,而应使用脉搏血氧仪来准确评估患者的血氧饱和度。
患者出现疾病的性质可能使低氧血症成为可能的结果,从而促使仔细临床寻找紫绀的证据,辅以紧急脉搏血氧仪。这种情况适用于许多常见的急性疾病,如心力衰竭,COPD恶化,肺炎和肺栓塞。一项对2276名肺炎患者的研究表明,低氧血症与六个危险因素独立相关:年龄> 30岁(OR 3.2),COPD(OR 1.9),充血性心力衰竭(OR 1.5),呼吸频率> 24 / min(OR 2.3) ),改变精神状态(OR 1.6)和胸部影像学浸润涉及> 1肺叶(或2.2)。36患有严重低氧血症的急性病患者可能会出现脉搏率或呼吸频率增加,因此通常会得到几个新点。 ,95 ,163 ,165 ,169
呼吸频率是严重疾病的唯一最佳预测因子。95然而,许多患者具有显着的低氧血症可以呈现与非特异性的研究结果如躁动和混乱,而不是呼吸困难,和氧饱和度已被证明是死亡率的紧急医疗接诊的结果的多变量分析的独立预测因子。19 ,170此外,鹅口疮的工作等人171对正常志愿者的研究表明,心率,血压和呼吸频率都不是低氧血症的可靠指标,低至饱和水平低至70%。这表明在大多数缺氧患者中观察到的生命体征的变化是由于潜在的疾病而不是低氧血症本身。
低氧血症可能与通气量增加或减少有关。虽然一些低氧血症患者可能会降低通气水平作为致病因素,但大多数低氧血症患者增加了每分钟通气量以增加血氧水平。例如,尽管肺部结构正常,但阿片类药物过量的患者可能会减少通气导致低氧血症,而肺炎或严重肺栓塞的患者可能由于V / Q不匹配而出现明显的低氧血症,尽管通气水平增加。尽管有明显的通气不足和低氧血症,但本例中的第一位患者可能看起来很平静且没有疼痛,而第二位患者可能会增加通气和心动过速。
完成患者的病史和快速评估后,更详细的体格检查可能会发现疾病的迹象,如严重的胸腔积液,严重的气胸或意外的心力衰竭,可能促使临床医生预测是否存在低氧血症。
对疑似低氧血症患者进行临床评估的良好实践点
应尽可能在急性呼吸困难的患者中进行病史,并且可能指出特定急性疾病的诊断,例如肺炎或肺栓塞或慢性病如COPD,哮喘或心力衰竭的恶化。
永远不要停止氧疗,以便在明显需要氧疗的患者的室内空气中进行血氧测量。
应紧急进行体格检查。这可能提供特定诊断的证据,例如心力衰竭或大量胸腔积液,但是直到胸部X光片等检查结果可用之前,仍然未确诊呼吸困难的原因。
通过脉搏血氧仪(SpO 2)测量记录的动脉血氧饱和度,并考虑不明原因混淆和激动的患者的血气评估,因为这可能是低氧血症和/或高碳酸血症的特征(紫绀是一种难以自信地记录的体征,特别是在贫困中轻或患有贫血或多尿症的病人)。
仔细测量呼吸频率和心率,因为在低氧血症患者中,痉挛和心动过速比紫绀的身体发现更常见。
应对任何“跟踪和触发”系统进行适当的更改,以便在有高碳酸血症呼吸衰竭风险的患者中实现较低的目标范围。如果在目标范围内,这些患者的饱和度应该没有EWS点,如果氧饱和度低于目标范围,或者在呼吸氧气时饱和度超过目标范围,则应该得分。2017年更新的NEWS图表有一个特殊的血氧测量测量部分,用于目标范围为88-92%的患者,建议所有医院都应使用2017年新闻图表(见建议B4)。
正常SpO 2的存在并不否定对血气测量的需要,特别是如果患者正在进行补充氧疗。在具有正常氧张力(PO 2)但异常二氧化碳张力(PCO 2)或由于贫血导致的低血氧含量的患者中脉搏血氧测定法将是正常的。出于这个原因,在这些测量可能影响患者结果的所有情况下,需要尽早进行血气和全血细胞计数测试。
所有使用血氧计的临床工作人员必须接受使用培训,并了解血氧测定的局限性。(血氧测定法是一种有价值的临床工具,但受人工制品和解释错误的影响)。
脉搏血氧测定法的出现彻底改变了低氧血症的临床评估,其方式与通过血压计的发明转化血压的临床评估大致相同。然而,过去常见的是患有急性呼吸道疾病的患者,他们已经进行过多次血压测量,但没有记录他们的氧饱和度,呼气峰值流量或FEV 1。除了未评估的临床后果之外,Howes 等172和Macnab 等[ 173]据报道,脉搏血氧仪的使用具有极高的成本效益,因为许多患者正常血氧测定(> 94%)的发现使得护理人员不常使用氧气,每个潜在的经济节省高达2324美元(~1200英镑)每年救护车。现在可用于高度便携,低成本的脉搏血氧仪应该可以在许多临床情况下测量氧饱和度,并将其用作“第五个生命体征”。我们鼓励所有参与急症患者护理的临床工作人员携带和使用一个,以便测量氧饱和度正常,这是患者听胸部评估的一部分。
脉搏血氧仪通过检测对应于氧合血红蛋白和脱氧血红蛋白的吸收峰的两个特定波长的光吸收来测量血红蛋白氧饱和度。在低饱和度(例如80%)下,血氧计不太可靠,但现代血氧计在饱和度高于约88%时准确地反映了SaO 2。174-178在本指南涵盖的几乎所有临床情况中,饱和度低于88%的患者将接受强化治疗,使饱和度达到至少90%,因此仪器在极低饱和度水平下的不准确性不应影响病人管理。
在一项对123名同时测量脉搏血氧饱和度和ABO测量的SaO 2的成年患者的研究中,中位差的95%CI范围为-0.6至+ 0.5%。176据估计,通过脉搏血氧仪测得的92%或更高的氧饱和度对于排除低氧血症的敏感性为100%,特异性为86%,定义为低于60 mm Hg(8 kPa)的动脉氧分压。179
在ICU的急性病患者中,血氧测定可能不太准确,但与稳定患者和健康个体相比,没有直接比较危重患者的脉搏血氧测定的准确性。Perkins 等人180的研究显示,平均SpO 2为94.6%,而平均SaO 2为95.9%,来自IC32的1132同时血氧计和ABG测量。幸运的是,脉搏血氧仪读数的平均差异为1.3%,因此在大多数情况下允许安全范围。该研究还表明,通过血氧测定法测量的氧饱和度的波动倾向于大于使用来自留置桡动脉导管的样品测量的SaO 2的变化。
虽然血氧测定法被广泛使用,但很少有临床研究检验其效用。Cochrane使用血氧测定法对超过20 000名患者进行围手术期监测的荟萃分析未能显示使用血氧测定法的并发症或死亡率的任何减少,尽管使用脉搏血氧仪监测的患者更常使用氧气。181作者认为,适度低氧血症的纠正可能对临床结果没有太大影响。
脉搏血氧仪不提供有关pH,PCO 2或血红蛋白水平的信息。因此,在这些测量可能影响患者结果的所有情况下,需要尽早进行血气和全血细胞计数测试。
外周灌注不良的患者脉搏血氧饱和度的准确性会降低,这些患者可能在系统性硬化症等慢性病或长期低血压或低血容症患者中长期发生。然而,有人建议许多类型的血氧计可以在低至20 mm Hg的动脉压下保持准确,只要机器能够在低脉冲压力下获得读数。182大多数血氧计给出脉搏信号强度的指示。重要的是确保血氧计在技术上可行时具有良好的信号,并且可能需要在不同的手指或脚趾上或在耳垂上尝试探针以获得针对个体患者的最佳可用信号。有些患者灌注不良,无法进行脉搏血氧饱和度测量。这包括患有严重外周的患者(例如,雷诺现象),严重的低血压和外周的“关闭”。
必须记住,在大多数贫血患者中,血氧测定法可以正常读取氧饱和度,因为可用血红蛋白的氧饱和度是正常的,尽管可用于氧运输的血红蛋白总量减少了。尽管患有“贫血性缺氧”,这些患者的氧饱和度水平正常,这可能导致血液中总氧含量显着降低。通常不认为SpO 2为98%但血红蛋白为7 g / dL((7×0.98×1.34)= 9.2 mL O 2 / dL)的患者血氧含量会大大降低。血红蛋白浓度为15 g / dL,饱和度为85%((15×0.85×1.34)= 17 mL O 2的患者/ dL的; 完全饱和时每g / dL血红蛋白携带1.34 mL氧气)。
在存在一氧化碳或高铁血红蛋白的情况下,血氧测定的准确性是不可靠的。这两种物质都具有与氧合血红蛋白相似的光吸收特性,因此患有一氧化碳中毒或高铁血红蛋白血症的患者中明显正常的SpO 2可能会错误地让人放心。血红蛋白水平高于2%可能导致SpO 2测量错误升高。183吸烟后不久,许多吸烟者的碳氧血红蛋白水平会高于这个水平,一些吸烟者的血红蛋白水平可能会升高到15%,而急性一氧化碳中毒则会升高到50%或更多。目前尚不清楚吸烟者在吸烟后几小时内发生突发疾病的血氧含量是否会降低对临床结果的影响,或者重度吸烟者是否可能在第一次吸烟者中获得比非吸烟者略高的目标饱和度范围。几个小时的严重疾病,以维持类似的血氧含量。
皮肤色素沉着也可能影响脉搏血氧饱和度读数的准确性(通常过高估计但有时低估)。特别是,在饱和度低于80-85%的深色皮肤参与者中,脉搏血氧饱和度的准确性受损。184-186然而,如果饱和度维持在本指南建议的范围内(大多数患者为94-98%),这在临床实践中很少成为问题,尽管Jubran和Tobin 31对通气参与者的工作表明在通气白人中,氧饱和度为92%可用于预测PaO 2高于60 mm Hg(8 kPa),但对于有时患有SpO 2的通气黑人参与者则不太可靠读数比直接测量的PaO 2高4%以上。在镰状细胞危象的情况下,脉搏血氧仪可能低估了氧合水平。187在这些情况下,阅读不足比阅读更安全,因为没有真正的低氧血症患者会被拒绝接受氧疗。在镰状细胞的患者,一项研究发现,镰状细胞危象期间脉搏血氧仪没有误诊要么低氧血症或normoxaemia提供了良好的波信号是目前,188血氧饱和度之间,但差异2和通过共血氧饱和度测量(SO 2)具有在镰状细胞危机期间被其他人发现189和稳定的患者。190在这些研究中,SpO2通常低于SaO 2,因此当没有镰状细胞患者时,脉搏血氧仪可能误诊低氧血症。
血氧计可能会受到患者手部运动的影响,但现代血氧计的问题比使用旧设备的问题要小。191运动伪影是更成问题的,如果患者还具有降低的被测定部位的灌注。192错位的血氧计传感器可能会导致人工制品过高估计或低估真正的氧饱和度; 这在患病患者的重新定位期间可能是一个特殊的问题。193
血氧测定的位置也很重要。手指和耳垂测量比应用于脚趾的探针的测量更准确,并且手指探针可能比耳探针更准确。194 ,195最后,医务人员需要记住除去指甲油和假指甲,避免血氧测量文物。
证据陈述
在大多数参与者中,脉搏血氧计准确度在直接测量的SaO 2的 1-2%范围内,但在皮肤黑暗的参与者中误差(通常高估但有时低估)更大,特别是饱和度非常低(低于80-85%)(证据水平) 2+)。
血氧计在休克,败血症和低血压中的准确性在很大程度上是未知的,但是大多数误差可能导致错误的低读数,这将导致额外的氧气被给予。因此,血氧测定中的大多数错误不太可能使患者处于危险之中,但重要的是确保血氧计具有良好的信号并避免由于运动,指甲油或其他潜在的错误来源造成的假象(证据级别3)。
建议睡眠患者的血氧饱和度测量应记录几分钟,以避免因氧饱和度正常的短暂夜间性浸润而被误导,如果睡眠期间注意到饱和度,临床医生应寻找打鼾或睡眠呼吸暂停的证据(证据)等级4)。
脉搏血氧仪在吸烟者中可能会误导正常,因为血液中的血红蛋白水平升高会导致血氧含量降低,尽管血氧饱和度明显正常且PO 2正常。因此,在过去10小时内吸烟的患者可能患低氧血症的风险增加(证据级别3)。
没有关于这些观察性研究的实施的对照试验,以下建议基于专家意见(证据级别4)。
建议
B2:氧饱和度,“第五个生命体征”,应由经过培训的工作人员使用脉搏血氧仪检查所有呼吸困难和急性病患者(必要时补充血气),并在观察时记录吸入氧气装置和流速血氧测定结果图表(D级)。
B3:急性不适患者的初步临床评估和随后的监测应包括使用公认的生理“追踪和触发”系统,例如可能由于低氧血症引起的临床检查,需要补充氧气或其他原因的新闻(等级) d)。BTS
B4:对于有高碳酸血症呼吸衰竭风险的患者,建议使用2017年新闻图表的相关部分。如果氧饱和度低于或高于目标范围(D级),则授予积分。
ABG是评估呼吸衰竭的“黄金标准测试”。然而,已发表的研究表明,来自耳垂(但不是来自手指)的动脉化毛细管气体可以提供与动脉样本几乎相同的pH和PCO 2的评估(血气采样的指示在章节中给出) 8.4和建议13)。196-200在急性和稳定情况下,耳垂标本进行的PO 2测量值比同时动脉测量值低0.5-1 kPa(3.7-7.5 mm Hg),大部分发散发生在PO 2高于8-10 kPa( 60-75毫米汞柱)。197 ,200这意味着大多数患者可以根据从耳垂血气中测量的pH和PCO 2水平进行安全管理,并通过脉搏血氧仪测量氧饱和度。197 ,200在危重病人,最初的样本应该是一个动脉标本,以保证准确的初步评估,而毛细管气体是作为一个病人稳定监测血气的进步尤为重要。
同时进行动脉和耳垂样本的患者将耳垂穿刺程序评定为比动脉穿刺疼痛少得多。201然而,在ABG取样之前局部麻醉的施用导致疼痛显着减少。202 ,203最近的随机试验发现,动脉穿刺使用胰岛素针引起较少的疼痛并减少手术并发症与标准针相比较。204
用胰岛素针穿刺的100 mm视觉模拟评分平均值(±SD)测得的疼痛评分低于标准针(23±22 vs 39±24 mm;平均差= -15 mm; 95%CI -22 mm至-7 mm; p <0.001)。然而,由于溶血率较高,作者建议胰岛素针的使用应限于在同一血液样本中不需要同时钾值的条件。
动脉穿刺造成动脉损伤的风险非常小,特别是如果使用桡骨部位。大多数关于手部缺血的报告涉及留置桡动脉插管,但也可能因针刺而损伤血管。205因此,该指南建议动脉化的耳垂标本应比现在更广泛地使用,作为ABG取样的更安全,更少痛苦的替代方法,并且应尽可能使用局部麻醉剂进行ABG取样,但这在医疗紧急情况和血液中通常不实用在这些情况下不应延迟气体采样。然而,耳垂样本在休克或低血压中的准确性尚不清楚,建议在所有休克或低血压(收缩压<90 mm Hg)的情况下使用ABG。
用于动脉化毛细管气体的患者准备,样品采集和样品处理技术非常复杂,只能由经过全面培训的人员进行。毛细管气体非常容易出现技术错误,只能在工作人员接受过充分使用培训的单位中进行紧急使用。有关静脉血气的建议,请参阅第7.2.3节。
使用动脉化毛细血管血气测量的证据陈述
患者发现耳垂标本比没有局部麻醉的动脉穿刺疼痛少(证据级别2 ++)。
ABG取样引起疼痛,可以通过在试验前使用局部麻醉剂来减轻疼痛(证据级别1+)。
动脉化的耳垂血气将提供关于PaCO 2和pH的准确信息,但不提供关于PO 2的准确信息(证据级别1-)。
耳垂标本给出的PO 2测量值比同时动脉测量值低0.5-1 kPa(4-7.5 mm Hg),氧气水平高于8-10 kPa(60-75 mm Hg)时出现更大的偏差(证据级别1- )。
However, a combination of earlobe gases (to monitor pH and PCO2) and oximetry (to measure oxygen levels) will allow safe management of most patients, even in emergency settings. (The only published evidence is for patients with COPD but this finding is likely to be generalisable to most patients other than those with shock or poor peripheral circulation) (evidence level 4).
The technique of patient preparation, sample acquisition and sample processing for arterialised capillary gases is complex and should only be undertaken by fully trained staff (evidence level 4).
Recommendations for use of ABGs and arterialised capillary blood gases
C1: For critically ill patients or those with shock or hypotension (systolic blood pressure <90 mm Hg), the initial blood gas measurement should be obtained from an arterial sample. For most patients who require blood gas sampling, either ABGs or arterialised earlobe blood gases may be used to obtain an accurate measure of pH and PCO2. However, the PO2 is less accurate in earlobe blood gas samples (it underestimates the PO2 by 0.5–1 kPa) so oximetry should be monitored carefully if earlobe blood gas specimens are used and a repeat arterial specimen should be taken if there is any concern about the accuracy of a capillary sample (grade D).
C2: Local anaesthesia should be used for all ABG specimens except in emergencies (grade A).
Transcutaneous oxygen devices give different information from pulse oximetry. They are more sensitive to reduced perfusion and may be used to monitor tissue oxygenation in trauma patients but their use is beyond the scope of this guideline.206
In patients with lung disease, hypercapnia may be accompanied by visible respiratory distress, but this will be absent when hypercapnia is a consequence of a reduction in minute ventilation. Patients may have a flushed face, a full and bounding pulse and muscle twitching together with the characteristic flap of the outstretched hands. In severe cases, consciousness may be depressed and convulsions may occur.
Gross hypercapnia usually occurs with profound hypoxaemia and it is therefore difficult to disentangle the direct effect of hypercapnia per se. Coma will usually occur when the PaCO2 is in the range 12–16 kPa (90–120 mm Hg). Survival has been seen following a PaCO2 of 67 kPa (500 mm Hg).207
The presence of hypercapnic respiratory failure can be anticipated in patients with severe exacerbations of COPD or other diseases such as severe neuromuscular disorders. Carbon dioxide is a vasodilator so patients with hypercapnia may develop headache. Carbon dioxide in high concentrations has hypnotic effects and patients with hypercapnia may progress from drowsiness with flapping tremor to confusion to coma.84 ,130–134 A study of 127 episodes of acute respiratory acidosis showed that the best clinical predictors of respiratory acidosis were drowsiness (OR 7.1), flushing (OR 4.1), the presence of known COPD (OR 3.3) and the presence of intercostal retraction (OR 2.9).208
Clinical symptoms and signs of carbon dioxide retention include:
Headache.
Poor appetite.
Vasodilation producing flushing and warm peripheries with dilated blood vessels (including retinal veins).
Bounding pulse.
Drowsiness.
Flapping tremor.
Confusion.
Coma.
Arterial or arterialised earlobe capillary blood gases will give an accurate estimation of pH and PaCO2 (see section 7.1.3 for further details).196–198 The blood gases will need to be repeated in 30–60 min in patients with significant hypercapnia or acidosis to monitor the response to treatment. Patients with COPD who remain acidotic despite 30–60 min of standard treatment (including targeted low-concentration oxygen therapy) are likely to need NIV.209
It has been suggested that the venous PCO2 level can be used to screen for hypercapnia in patients with acute respiratory disease. A study of 196 paired samples of arterial and venous blood from patients with acute respiratory disease showed that the PCO2 in the venous sample was an average of 0.77 kPa (5.8 mm Hg) higher than the simultaneous arterial sample.210 A venous PCO2 below 6 kPa (45 mm Hg) had 100% sensitivity for eliminating the risk of hypercapnia (arterial PCO2 above 6 kPa or 45 mm Hg), although the specificity was low at 57% and there was more variation in some studies.211–213 For patients who are not at risk of metabolic acidosis, the presence of a satisfactory oxygen saturation measured by pulse oximetry and a venous PCO2 below 6 kPa (45 mm Hg) can exclude the possibility of significant arterial hypoxia or hypercapnia and may obviate the need for ABG measurements. This advice is strengthened by a recent prospective cohort study and a meta-analysis of five previous studies.214 ,215 Although the use of venous PCO2 is becoming more common, it is still not widely enough used in clinical practice for the guideline committee to make a clear recommendation on its use.
Waveform capnography to assess end-tidal CO2 is used primarily to confirm tracheal intubation during anaesthesia, intensive care and for any patients requiring endotracheal intubation. They are considered the ‘gold standard’ by the Royal College of Anaesthetists. The absence of any detectable carbon dioxide output indicates a failed intubation. The management of intubated patients is outside the remit of this guideline.
Waveform capnography monitors are also useful in the management of cardiac arrest and circulatory collapse. Waveform capnography during CPR allows: (1) confirmation of correct tracheal tube placement; (2) monitoring of the respiratory rate; (3) assessment of CPR quality—improved chest compression quality results in increased end-tidal CO2 level; (4) indication of return of spontaneous circulation (ROSC)—a large increase in end-tidal CO2 during CPR can indicate ROSC; (5) a very low end-tidal CO2 value during CPR despite high-quality chest compressions is associated with a low probability of ROSC.216–218 These devices are also useful in the care of intubated patients in the emergency department because, through visualising a typical ‘box wave form’, they can confirm that the tube is in the airway even in the absence of carbon dioxide production during a cardiac arrest. A sudden increase in carbon dioxide may be the first sign of spontaneous circulation.219
End-tidal carbon dioxide measurements correlate poorly with arterial carbon dioxide levels in patients with COPD, but they may be useful in some research studies of hyperventilation syndromes. However, these devices are inaccurate in patients with airways disease and those with a high respiratory rate, so they should not be used in the management of patients with respiratory failure and they will not be discussed further in this guideline.
The recent availability of portable devices to measure transcutaneous partial pressure of carbon dioxide (PtCO2) at the bedside provide a promising alternative to an ABG. They function on the principle that CO2 diffuses extremely well through tissues. A probe is attached to an area of skin (usually the earlobe) and warms to 42°C which ‘arterialises’ the underlying capillaries. The CO2 diffusing through the skin changes the pH of a thin electrolyte membrane in the probe and the resulting signal is converted to an estimate of the PaCO2. As well as measuring PtCO2, the probe also measure SpO2. Early studies indicate that such devices can be accurate in normal volunteers. Transcutaneous CO2 devices have provided accurate estimates of PaCO2 in a variety of clinical scenarios including AECOPD, invasive and NIV in ICUs and overnight studies of sleep-disordered breathing.220–224
Recently transcutaneous CO2 monitoring has been used in the emergency department in patients presenting with acute severe asthma136 and community-acquired pneumonia225 The PtCO2 accurately assessed PaCO2 as measured by the ‘gold standard’ ABG.226 A rise in PtCO2 was demonstrated in both groups of patients on administration of high-flow oxygen for 60 min, the significance of this will be discussed further in section 8.12. These new techniques are not yet recommended for routine clinical use.
Tables 1⇑⇑–4 are based on section 8, they are shown at the front of the guideline.
The hospital management of hypoxaemic patients is presented before the prehospital management. Some readers may prefer to read section 9 (prehospital care) first because most patients receive prehospital care before hospital care, but the Guideline Development Group preferred to present the hospital management first because a wider range of therapeutic options and a fuller range of investigations such as blood gas results are available in the hospital environment than in most prehospital settings.
Breathless patients may arrive in hospital directly (without prior assessment) or in ambulances where they will usually have been assessed by paramedics who may also have initiated emergency treatments including oxygen therapy. As discussed in section 7 of this guideline, assessment, triage and resuscitation of critically ill patients must be undertaken in parallel with the initiation of oxygen therapy and specific treatment must be given for the underlying medical condition. All critically ill patients and all patients at risk of hypercapnic respiratory failure should be triaged as very urgent and should have blood gases taken on arrival in hospital. Furthermore, all seriously ill patients should be assessed by senior clinicians in the emergency department as early as possible. In many cases, this may involve liaison with intensive care specialists or with appropriate other specialists who can deal effectively with the patient's major medical or surgical problems.
Readers are referred to section 7.1.1 and to disease-specific guidelines for advice concerning the immediate assessment and management of seriously ill patients.
Readers are referred to section 10 for advice concerning choice of oxygen delivery devices and systems.
Readers are referred to tables 1⇑⇑–4 and charts 1 and 2 in the introductory section for a summary of the key elements of oxygen therapy in common medical emergencies.
Remember to ask for senior and specialist advice early in the care of profoundly ill patients.
Clinicians must bear in mind that supplemental oxygen is given to improve oxygenation, but it does not treat the underlying causes of hypoxaemia which must be diagnosed and treated as a matter of urgency.
The immediate management of medical emergencies in hospital settings before blood gas results are available is similar in principle to management in the prehospital setting (section 9). The main priorities are to avoid harmful levels of hypoxaemia for all patients and to avoid harmful levels of hypercapnia for patients who are at risk of this complication. However, the amount of information available to the healthcare professionals increases rapidly in the hospital environment. The hospital management is presented before the prehospital management because it represents the ‘ideal’ management. This may also be achievable in some prehospital settings such as a well-equipped primary care centre and in some ambulance settings such as ambulances with critical care outreach facilities. However, in many prehospital settings there will usually be less information available concerning a patient's history and physiology and less equipment available to assess and treat the patient.
Differences between hospital settings and prehospital settings include:
Pulse oximetry is almost always available in hospital at present. These guidelines also recommend that pulse oximetry must be available in all locations where emergency oxygen is used (section 9.1).
Blood gas results can be available within minutes of arrival in hospital.
Additional diagnostic information may be available from history, clinical examination, test results and from the patient's hospital records.
Additional equipment and resources are available.
Because of the universal availability of oximetry in hospitals, it is rare for the hospital medical team to have to administer oxygen on the basis that a patient ‘might be hypoxaemic’. However, initial ‘blind management’ is sometimes necessary for patients with shock or with very poor peripheral circulation where a reliable pulse oximetry trace cannot be obtained. ABGs should be obtained as a matter of urgency in all such cases.
Supplemental oxygen therapy is recommended for all acutely hypoxaemic patients and for many other patients who are at risk of hypoxaemia, including patients with major trauma and shock. Many acutely breathless patients will require supplemental oxygen therapy, but there are some situations such as acute hyperventilation or diabetic ketoacidosis where an apparently breathless patient will not benefit from oxygen therapy. There are some other clinical situations such as carbon monoxide or cyanide poisoning where a patient may benefit from oxygen therapy despite an apparent lack of hypoxaemia or breathlessness because carbon monoxide binds more avidly than oxygen to the haemoglobin molecule and cyanide poisoning leads to histotoxic hypoxia. Carbon monoxide poisoning and cyanide poisoning often coexist in patients suffering from smoke inhalation.227
Although it is well recognised that profound hypoxaemia can lead to organ failure and death, it would be unethical to undertake randomised studies involving the deliberate exposure of acutely ill patients to severe hypoxaemia so most recommendations are based on expert opinion unless otherwise stated.
Oxygen saturation should be measured in all breathless and acutely ill patients as discussed in recommendation 9 and oxygen therapy should be given to hypoxaemic patients as described in tables 1⇑⇑–4 and recommendations 1–4. Patients do not require oxygen therapy if their oxygen saturation is 94% or above (exceptions are carbon monoxide poisoning, cyanide poisoning and pneumothorax; see sections 8.10.7 and 8.11.6). Patients on oxygen with SpO2>98% (with the above exceptions) do not usually require oxygen therapy or may require a lower concentration. All patients with shock, major trauma, sepsis or other critical illness should be managed initially with high-concentration oxygen therapy from a reservoir mask. Targeted oxygen therapy can be initiated once there is spontaneous circulation and oximetry can be measured reliably (see table 1 and recommendations E1–E2).
Blood gases should be measured as soon as possible in most emergency situations involving hypoxaemic patients228 and are essential in patients who may develop hypercapnic respiratory failure (carbon dioxide retention with risk of respiratory acidosis). This includes all patients admitted with an AECOPD, even in the absence of hypoxaemia.1 Blood gases should also be checked (and the clinical situation should be reviewed) if the oxygen saturation should fall by more than three percentage points, even if the saturation remains within the target range. For example, a fall from 98% to 94% might be due to a significant event such as a pulmonary embolus. In this situation, the saturation of 94% will not harm the patient but the patient will remain at serious risk until the pulmonary embolism is diagnosed and treated. If oximetry shows a patient to be hypoxaemic, the initiation of oxygen therapy should not be delayed while awaiting the results of blood gas measurements.
Blood gas measurements are not usually required for patients with no risk factors for hypercapnic respiratory failure and an oxygen saturation of 94% or above breathing air unless the patient requires blood gas estimation for other reasons such as suspected metabolic acidosis or diabetic ketoacidosis. The BTS asthma guideline recommends that ABG measurements need not be undertaken in patients with acute asthma and an oxygen saturation above 92% and no life-threatening features.229 ABG sampling can be technically difficult, especially for poorly perfused patients, and junior staff should ask for assistance from more senior staff in difficult cases.
Following initial clinical assessment and the availability of a pulse oximetry measurement, a decision can be made regarding the need for blood gas estimation within a few minutes of arrival in the hospital environment or if a previously stable patient develops breathlessness within a hospital environment. Oximetry will give no information concerning carbon dioxide or pH levels and a normal pulse oximetry level may provide false reassurance in patients on oxygen therapy who may have unexpected hypercapnia and acidosis. However, careful clinical assessment supplemented by the use of oximetry will allow the setting of an appropriate oxygen saturation target for different groups of patients until blood gas results are available.
If repeated blood gas estimations are required, the timing will depend on the indication. In general, the oxygen saturation (and PO2) stabilises at a new higher level within a few minutes of increasing the concentration of oxygen but the PaCO2 can take 30–60 min to equilibrate. The rise in blood oxygen level can be monitored with oximetry, so repeat blood gas tests are performed mostly to assess critical illness (immediate sampling required) or to monitor pH and PCO2 levels (best performed 30–60 min after increasing the concentration of oxygen).
Evidence statement:
The use of blood gases in acute illness is guided by observational data and expert opinion (evidence level 4).
Recommendation
C3: Blood gases should be checked in the following situations
All critically ill patients (grade D).
Unexpected or inappropriate fall in SpO2 below 94% in patients breathing air or oxygen or any patient requiring oxygen to achieve the above target range (grade D). (Allowance should be made for transient dips in saturation to 90% or less in normal participants during sleep.)
Deteriorating oxygen saturation (fall of ≥3%) or increasing breathlessness in a patient with previously stable chronic hypoxaemia (eg, severe COPD) (grade D).
Most previously stable patients who deteriorate clinically and require increased FiO2 to maintain a constant oxygen saturation (grade D).
Any patient with risk factors for hypercapnic respiratory failure who develops acute breathlessness, deteriorating oxygen saturation, drowsiness or other features of carbon dioxide retention (grade D).
Patients with breathlessness who are thought to be at risk of metabolic conditions such as diabetic ketoacidosis or metabolic acidosis due to renal failure (grade D).
Any other evidence from the patient's medical condition that would indicate that blood gas results would be useful in the patient's management (eg, an unexpected change in ‘track and trigger’ systems such as a sudden rise of several units in the NEWS or an unexpected fall in oxygen saturation of 3% or more, even if within the target range) (grade D).
Readers are referred to section 7.1.3 for advice concerning when to use ABGs and when to use arterialised capillary blood gases.
In the past, oxygen was prescribed at a fixed FiO2 or at a fixed flow rate via nasal cannulae or variable performance face masks. However, several audits have shown that many (or most) patients did not receive the prescribed concentration of oxygen when this methodology was used.4–10 Furthermore, a patient's oxygen requirement may vary over time so the prescribed oxygen concentration may be too high or too low even a short time after the prescription was written. For this reason, it is recommended that oxygen should be prescribed to a target saturation range rather than prescribing a fixed concentration of oxygen or FiO2. This is analogous to an insulin ‘sliding scale’ where the prescriber specifies a variable dose of insulin to achieve a target blood glucose range rather than prescribing a fixed dose of insulin. This will allow the appropriate healthcare professional—usually a doctor, registered nurse or physiotherapist—to adjust each patient's concentration of oxygen to achieve the safest oxygen saturation range for each patient.
The prescriber may indicate a starting concentration, device or flow rate, but there needs to be an agreed system for adjusting the oxygen concentration upwards or downwards according to a patient's needs (see charts 1 and 2; sections 11.3.6 and 11.3.7 and figure 19). As a patient improves, he or she is likely to require a lower FiO2 over a time period that will vary between patients. Most recovering patients will eventually require no supplemental oxygen. On the other hand, a deteriorating patient may need an increased concentration of oxygen. This increase can be initiated by registered nursing staff or physiotherapists.
Good practice points
The requirement for an increased concentration of oxygen is an indication for urgent clinical reassessment of the patient (and repeat blood gas measurements in most instances). See recommendations W13 and W15 for exceptions.
Oxygen should be prescribed to a target saturation range rather than prescribing a fixed concentration of oxygen or FiO2 (see recommendations A1, A2, A4 and A5).
It is recommended that all patients admitted to hospital should have a prescription for an oxygen target range set at the time of admission, ideally as part of an ‘admission bundle’ which may include other key elements such as thromboprophylaxis and MRSA prevention. This will ensure that the correct amount of oxygen will be administered while awaiting full medical assessment if the patient should deteriorate unexpectedly at any time during the hospital admission.
As discussed in sections 4–6 of this guideline, there is no evidence of benefit from above normal oxygen saturation in most clinical situations and there is evidence that excessive concentrations of oxygen can have adverse effects, even in some patients who are not at risk of hypercapnic respiratory failure. A target oxygen saturation range of 94–98% will achieve normal or near-normal oxygen saturation for most patients who are not at risk of hypercapnic respiratory failure. Furthermore, the suggested lower limit of 94% allows a wide margin of error in the oximeter measurement, thus minimising the risk of any patient being allowed to desaturate below 90% due to inaccurate oximetry.
Patients with critical illness requiring high-concentration oxygen therapy are discussed in section 8.10.
Patients with medical emergencies which frequently cause breathlessness and hypoxaemia are discussed in section 8.11.
Patients with COPD and other conditions that may predispose to hypercapnic respiratory failure are discussed in section 8.12.
Medical emergencies for which oxygen was commonly given in the past but is not actually indicated unless the patient is hypoxaemic are discussed in section 8.13.
As soon as blood gas measurements are available, a patient's further treatment can be guided by the results of this test. For patients with a normal or low PCO2 and no risk factors for hypercapnic respiratory failure, it is safe to aim at an oxygen saturation in the normal range (94–98%). For patients with a raised PCO2, a lower oxygen saturation is indicated (88–92%), especially if the patient is acidotic. NIV is recommended for patients with COPD who have hypercapnia and a pH<7.35 ([H+] >45 nmol/L) despite 1 hour of standard medical treatment including controlled oxygen therapy.1 ,209
The technical and practical aspects of different oxygen delivery systems are discussed in section 10. For major trauma cases and for severely hypoxaemic patients without risk factors for hypercapnic respiratory failure, a non-rebreathing mask (reservoir mask) at 15 L/min is the suggested first choice. The delivery system and FiO2 may be adjusted later to a lower concentration of oxygen as a patient improves or towards supported ventilation if the patient deteriorates. The majority of patients with modest hypoxaemia can be treated with nasal cannulae or a simple face mask at a flow rate which is adjusted to maintain the oxygen saturation in the target range for their specific clinical presentation. Chart 2 shows a suggested scheme that allows the oxygen level to be adjusted upwards or downwards in gradual increments depending on a patient's clinical progress (see also sections 11.3.6 and 11.3.7). Venturi masks were previously recommended for low-concentration oxygen therapy because they deliver a more reliable oxygen concentration than nasal cannulae or variable flow masks.230 They can also be combined with a humidifier system when necessary (see section 10.2.3). The mask and/or flow should be rapidly changed if the initial choice does not achieve the target saturation. However, the only randomised study of targeted oxygen therapy in AECOPD used nasal cannulae which have the advantage of being adjustable (by variation in flow rate) without having to change the device itself.51
High-concentration oxygen from reservoir mask (15 L/min) or when using a bag mask or advanced airways (supraglottic airway or tracheal tube) for assisted ventilation during respiratory arrest or during CPR.
Nasal cannulae (2–6 L/min) or simple face masks (5–10 L/min) for medium-concentration oxygen therapy (and HFNC using specialised equipment for high-concentration oxygen therapy, often as an alternative to a reservoir mask).
Twenty-four per cent Venturi mask at 2 L/min or 28% Venturi masks at 4 L/min for patients at risk of hypercapnic respiratory failure (alternatively use nasal cannulae at 1–2 L/min, especially when the patient has stabilised).
Tracheostomy masks for patients with a functioning tracheostomy (adjust flow to achieve desired saturation).
There are a number of major medical emergencies where patients are very likely to suffer from hypoxaemia. High-concentration oxygen therapy from a reservoir mask at 15 L/min is recommended in the initial management of all such patients prior to stabilisation and the availability of a reliable oximetry reading. Once this is achieved, the concentration of oxygen can be titrated downwards to maintain a target saturation of 94–98%. It is recommended that patients with COPD or other risk factors for hypercapnia who develop a critical illness should be treated by emergency services in the same manner as other critically ill patients until urgent blood gas results become available because the primary issue is the critical illness. Critically ill patients with hypercapnia, hypoxaemia and acidosis will require immediate assessment by intensive care teams and will usually require tracheal intubation and mechanical ventilation.
Evidence statement
The use of oxygen in major medical emergencies is guided by observational data and expert opinion (evidence level 4).
The 2015 guideline for Adult Advanced Life Support issued by Resuscitation Council UK recommends the use of the highest possible inspired oxygen level for ventilation during CPR; that guideline also makes recommendations regarding choice of airway and ventilation technique in these circumstances.231 The present guideline endorses these proposals during the period of resuscitation. Subsequent management will depend on the underlying condition and the patient's degree of recovery. There is theoretical evidence that patients with a ROSC may be managed more safely with a lower initial inspired oxygen than with 100% oxygen.98 ,99 Recently, in an observational study, Kilgannon et al151 ,152 reported increased mortality among survivors of cardiac arrest who had been exposed to very high levels of oxygen (PaO2>300 mm Hg or 40 kPa) in the first 24 hours on the ICU. Bellomo et al154 also found an excess of deaths in this group of patients but argued that the risk was no longer statistically significant after multivariate analysis. Elmer et al232 reported a small single-centre study in 2015 in which severe hyperoxaemia (PaO2>300 mm Hg or 40 kPa) was associated with increased hospital mortality but moderate hyperoxaemia (101–299 mm Hg) was not associated with decreased survival.
A systematic review and meta-analysis by Wang et al233 concluded that hyperoxaemia appears to be correlated with increased in-hospital mortality in survivors of adult cardiac arrest but the result should be interpreted cautiously because of the significant heterogeneity and the limited number of studies that were analysed.
Based on the above evidence, current UK and European Resuscitation guidelines recommend a target oxygen saturation of 94–98% once spontaneous circulation had been restored.231 This guideline endorses these recommendations.
Evidence statement
The use of oxygen during and after CPR is based on expert opinion and extrapolation from observational data (evidence level 4).
Recommendation
E1: Use the highest feasible inspired oxygen for ventilation during CPR (see table 1 and section 8.10). Once spontaneous circulation has returned and arterial blood oxygen saturation can be monitored reliably, aim for a target saturation range of 94–98% and take an ABG sample to guide ongoing oxygen therapy. If the blood gas shows hypercapnic respiratory failure, reset the target range to 88–92% or consider mechanical ventilation (grade D).
There is evidence that early intervention to normalise oxygen delivery to the tissues using volume expansion and vasoactive agents is beneficial in the management of critically ill patients with shock or sepsis, but there is no evidence of benefit from attempts to achieve supranormal oxygen delivery.73–75 ,234–238 In fact, there is evidence that hyperoxia can cause a paradoxical decrease in whole body oxygen consumption in critically ill patients,239 and it has been demonstrated that hyperoxia can impair oxygen delivery in septic patients.240 A study using a rat model of progressive haemorrhage found that both hypoxaemia and hyperoxaemia compromised haemodynamics. There was a paradoxical fall in tissue PO2 in hyperoxaemic animals despite the high PaO2.241 These factors may account for the observation by deJonge (but disputed by Eastwood) that mortality was elevated among intensive care patients who were hyperoxaemic during the first day on the ICU.153 ,155 In de Jonge's study of 36 307 patients on ICUs in the Netherlands, the adjusted OR for death was lowest in a PO2 range of 8.9–10.6 kPa (equivalent to saturation about 93–96% at normal pH). Two recent systematic reviews with meta-analysis have addressed this subject. Both studies concluded that hyperoxaemia was associated with increased hospital mortality but caution is required in interpreting the results because of heterogeneity in the included studies, including different definitions of hyperoxaemia.242 ,243 A randomised trial published in 2016 reported ICU mortality of 11.6% in 216 patients randomised to a target saturation range of 94–98% (median PaO2 11.6 kPa) compared with 20.2% mortality among 218 patients randomised to conventional therapy (median PaO2 13.6 kPa).244 The absolute risk reduction was 8.6% (risk reduction 0.086; 95% CI 0.017 to 0.150; p=0.01) and hospital mortality was 24.2% vs 33.9% (absolute risk reduction 0.099; 95% CI 0.013 to 0.182; p=0.03). However, the trial was prematurely terminated due to difficulty with recruitment, and the authors advise caution in interpreting the results for this reason.
Most critically ill patients are at risk of multiorgan failure and therefore require intensive care assessment as a matter of urgency. Critical care consensus guidelines set 90% saturation as the minimum level below which oxygen saturation should not be allowed to fall.31 ,32 ,245 The 2012 Surviving Sepsis Campaign guideline is mainly based on mixed venous oxygen saturation or central venous saturation but also recommends a target SaO2 of 88–95% for patients with sepsis.31 ,32 ,245 However, these recommendations are based on directly measured SaO2 in critical care settings with intensive levels of nursing and monitoring. The present guideline recommends a slightly higher target saturation range prior to the transfer of these seriously ill patients to critical care facilities.
For most critically ill or severely hypoxaemic patients, initial oxygen therapy should involve the use of a reservoir mask, aiming at an oxygen saturation of 94–98%. If the patient has concomitant COPD or other risk factors for hypercapnic respiratory failure, the initial saturation target should also be 94–98% pending the results of blood gas estimations and assessment by intensive care specialists. If critically ill patients with COPD have hypercapnia and acidosis, the correction of hypoxaemia must be balanced against the risks of respiratory acidosis and ventilatory support using NIV or invasive ventilation should be considered.
It is also recognised that many patients with long bone fractures may develop hypoxaemia even in the absence of injury to the airway or chest (possibly due to opioid treatment and fat embolism) and they should be monitored with oximetry and given oxygen if necessary.38 ,246–248 These patients, if not critically ill, should have a target oxygen saturation of 94–98% or 88–92% if they have coexisting COPD or other risk factors for hypercapnic respiratory failure.
Evidence statement
The use of oxygen in critical illness is based on expert opinion guided by physiology and observational data (evidence level 4).
Recommendation
E2: In critical illness, including major trauma, sepsis, shock and anaphylaxis, initiate treatment with a reservoir mask at 15 L/min and aim at a saturation range of 94–98%. This advice also applies to patients with critical illness who have risk factors for hypercapnia pending the results of blood gas measurements and expert assessment. In patients with spontaneous circulation and a reliable oximetry reading, it may be possible to maintain a saturation of 94–98% using lower concentrations of oxygen (grade D).
Survivors of drowning may have suffered inhalation of fresh or sea water into the lungs and may become hypoxaemic. Supplemental oxygen should be given to all patients with saturation below 94%, aiming at a target saturation of 94–98%.249
Evidence statement
The use of oxygen in drowning is based on expert opinion (evidence level 4).
Recommendation
E3: In cases of drowning, aim at an oxygen saturation of 94–98% once adequate circulation is restored (grade D).
Patients with anaphylaxis are likely to suffer from tissue hypoxia due to a combination of upper and/or lower airway obstruction together with hypotension. In addition to specific treatment of these problems, the Resuscitation Council UK recommends initial high-concentration oxygen (10–15 L/min, by reservoir mask) for patients with anaphylaxis.231 ,250 The present guideline would endorse this practice in the immediate management of anaphylaxis followed by a target saturation of 94–98% once the patient's oxygen saturation can be measured reliably.
Evidence statement
The use of oxygen in anaphylaxis is based on expert opinion (evidence level 4).
Major pulmonary haemorrhage and massive haemoptysis can occur for a large number of reasons ranging from acute pulmonary vasculitis to erosion of a blood vessel by a lung tumour. In addition to specific treatment of the causative condition, most such patients require supplemental oxygen treatment (also see table 1). A target saturation range of 94–98% is recommended. Treatment should be initiated with high-concentration oxygen via a reservoir mask and subsequently adjusted according to chart 2 to maintain a saturation of 94–98% pending the results of blood gas measurements.
Evidence statement
The use of oxygen in pulmonary haemorrhage is based on expert opinion (evidence level 4).
As this is a life-threatening condition where a patient may suffer from cerebral hypoxia (and oximetry may not be possible), patients with status epilepticus should be treated in accordance with table 1 (reservoir mask until clinically stabilised).
Evidence statement
There have been no clinical trials of oxygen use during epileptic fits and it may be impossible to obtain an oximetry signal in these circumstances. Expert opinion advises the administration of high-concentration oxygen until oximetry measurements can be obtained (evidence level 4).
Recommendation
E4: In patients with acute seizures due to epilepsy or other causes, high-concentration oxygen should be administered until a satisfactory oximetry measurement can be obtained and clinicians should then aim for an oxygen saturation of 94–98% or 88–92% if the patient is at risk of hypercapnic respiratory failure (grade D).
Patients with major head injury are at risk of hypoxaemia and hypercapnia. They require urgent assessment and maintenance of airway patency, either through positioning, simple adjuncts or early tracheal intubation and ventilation to avoid further brain injury due to brain oedema which may be aggravated by hypoxaemia and/or hypercapnia. These patients should be triaged directly where possible to a major trauma centre. Initial treatment should include high-concentration oxygen via a reservoir mask pending availability of satisfactory blood gas measurements or until the airway is secured by intubation which will also protect against the risk of aspiration due to reduced consciousness. Although hypoxaemia is common in patients with head injury (and associated with poorer outcomes), the relative contribution of hypoxaemia to outcome is not yet established.37 ,251–255 All authors agree that hypoxaemia should be corrected, but a review of the literature concluded that there is no evidence of clinical benefit from hyperoxia in brain injured patients and a subsequent clinical study showed that normobaric hyperoxia did not improve brain metabolism in five patients with acute severe brain injury.256 ,257 There are no UK guidelines for oxygen therapy in the immediate phase after head injury, but US guidelines recommend maintaining an oxygen saturation above 90% for patients with acute brain injury.30 An American study published in 2009 describes a cohort of 3420 patients and the authors reported worse outcomes in patients with severe traumatic brain injury associated with hypoxaemia and extreme hyperoxaemia. Outcomes were optimal in the PaO2 range of 110–487 mm Hg (14.6–65 kPa).258 Other observational studies have suggested that hyperoxaemia may be associated with improved outcomes. Asher et al259 recently reported the outcomes for 193 adult patients with severe traumatic brain injury who had overall survival of 57%. They reported that a PaO2 threshold between 250 and 486 mm Hg (33–65 kPa) during the first 72 hours after injury was associated with improved all-cause survival, independent of hypocarbia or hypercarbia. Two recent observational studies have provided further evidence that hyperoxaemia may be associated with increased mortality in traumatic brain injury.260 ,261 The present guideline advises giving supplementary oxygen if required to maintain an oxygen saturation in the range of 94–98% pending the publication of randomised studies comparing normoxaemia with normobaric hyperoxaemia.
Evidence statement
The use of oxygen in cases of major head injury is based on expert opinion and extrapolation from observational studies (evidence level 4).
Recommendation
E5: In cases of major head injury, aim at an oxygen saturation of 94–98%. Initial treatment should involve high-concentration oxygen from a reservoir mask at 15 L/min pending availability of satisfactory blood gas measurements or until the airway is secured by intubation (grade D).
Patients with carbon monoxide poisoning may have a normal level of PaO2 but a greatly reduced level of oxygen bound to haemoglobin because this has been displaced by carbon monoxide.262 Standard pulse oximetry cannot screen for carbon monoxide exposure as it does not differentiate carboxyhaemoglobin from oxyhaemoglobin and blood gas measurements will show a normal PaO2 in these patients. Some newer co-oximeters can measure carboxyhaemoglobin levels as well as SpO2.The blood carboxyhaemoglobin level must be measured to assess the degree of carbon monoxide poisoning. The half-life of carboxyhaemoglobin in a patient breathing air is ∼300 min; this decreases to 90 min with high-concentration oxygen via a reservoir mask. The most important treatment for a patient with carbon monoxide poisoning is therefore to give high-concentration oxygen via a reservoir mask. Comatose patients or those with severe mental impairment should be intubated and ventilated with 100% oxygen. The role of hyperbaric oxygen remains controversial. A 2011 Cochrane review concluded that existing randomised trials did not establish whether the administration of hyperbaric oxygen to patients with carbon monoxide poisoning reduced the incidence of adverse neurological outcomes.263 However, a randomised trial published in 2007 has suggested that patients with loss of consciousness or high carboxyhaemoglobin levels may have less cognitive sequelae if given hyperbaric oxygen.264
Evidence statement
The use of oxygen in carbon monoxide poisoning is based on expert opinion and extrapolation from observational studies (evidence level 4).
Recommendation
E6: In cases of carbon monoxide poisoning, an apparently ‘normal’ oximetry reading may be produced by carboxyhaemoglobin, so aim at an oxygen saturation of 100% and use a reservoir mask at 15 L/min irrespective of the oximeter reading and PaO2 (grade D).
Patients who present with acute medical emergencies who are not critically ill and who have saturation >85% can be treated with medium-concentration oxygen therapy from nasal cannulae or a simple face mask with a target saturation range of 94–98%. Some of these patients (eg, patients with pneumonia) may subsequently deteriorate, requiring high-concentration oxygen from a reservoir mask or requiring respiratory support such as invasive ventilation. Others may turn out to have an additional diagnosis of COPD or neuromuscular disease with a risk of hypercapnic respiratory failure and they should be managed with a 24% Venturi mask at 2–3 L/min or 28% Venturi mask at 4 L/min or 1–2 L of oxygen via nasal cannulae, aiming at a target saturation of 88–92%. There are no published trials supporting the use of oxygen to relieve breathlessness in non-hypoxaemic patients, and there is evidence from randomised studies that oxygen does not relieve breathlessness compared with air in non-hypoxaemic patients with COPD who are breathless following exertion or breathless palliative care patients with PO2>7.3 kPa or 55 mm Hg (saturation above about 88%).146 ,150
It is common for breathless and hypoxaemic patients to have no firm diagnosis at the time of presentation. For most acutely hypoxaemic patients whose medical problem is not yet diagnosed, an oxygen saturation range of 94–98% will avoid the potential hazards associated with hypoxaemia or hyperoxaemia (see sections 4–6 and tables 1–2). Aiming for an oxygen saturation in the normal range (rather than an abnormally high oxygen level) will also have the effect of allowing the lowest effective FiO2 to be used, thus avoiding risks such as absorption atelectasis and V/Q mismatch that may be associated with the use of very high fractions of inspired oxygen (see sections 5 and 6). The priority for such patients is to make a specific diagnosis as early as possible and to institute specific treatment for the underlying condition. Early blood gas measurement is mandatory in the management of patients with sudden unexplained hypoxaemia.
Evidence statement
The use of oxygen in most instances of acute hypoxaemia is guided by expert opinion based on physiology and observational studies except where indicated otherwise in the sections that follow (evidence level 4).
Recommendations
D1: For acutely breathless patients not at risk of hypercapnic respiratory failure who have saturations below 85%, treatment should be started with a reservoir mask at 15 L/min in the first instance (see figures 1–2 (charts 1–2) and table 2 and sections 8.10 and 10).* The oxygen concentration can be adjusted downwards (using nasal cannulae at 1–6 L/min or a simple face mask at 5–10 L/min) to maintain a target saturation of 94–98% once the patient has stabilised (grade D).
D2: In other cases of acute hypoxaemia without critical illness or risk factors for hypercapnic respiratory failure, treatment should be started with nasal cannulae (or a simple face mask if cannulae are not tolerated or not effective) with the flow rate adjusted to achieve a saturation of 94–98% (grade D).
D3: If medium-concentration therapy with nasal cannulae or a simple face mask does not achieve the desired saturation, change to a reservoir mask and seek senior or specialist advice (grade D).
Good practice point
High-flow nasal oxygen using specialised equipment should be considered as an alternative to reservoir mask treatment in patients with acute respiratory failure without hypercapnia.
*For initial management of patients at risk of hypercapnic respiratory failure, see recommendations G1 and G2.
The BTS/SIGN guideline for the management of acute asthma recommends that the oxygen saturation should be maintained between 94% and 98%.229 Although there is no danger of tissue hypoxia at any saturation above 90%, a drop of oxygen saturation below 94% may indicate deterioration and should prompt a further assessment. Supplemental oxygen should be started using nasal cannulae at 2–4 L/min or a simple face mask at 5 L/min or 35–40% Venturi mask and adjusted as necessary to maintain a saturation of 94–98%.265
A study which was published in 2003 showed that the administration of 100% oxygen to patients with acute severe asthma produced an increased PaCO2 and a decreased peak expiratory flow compared with patients treated with 28% oxygen.266 The authors of that study recommended the use of targeted oxygen therapy rather than giving high-concentration oxygen to all patients with acute severe asthma. This advice has been reinforced by the randomised study of Perrin et al136 who found a significant increase in transcutaneous PCO2 when oxygen was given at 8 L per minute via simple face mask. Of 106 patients randomised to high-concentration oxygen or targeted oxygen therapy (target 93–95%), all 10 instances of hypercapnia occurred in patients given high-concentration oxygen therapy. Hypercapnia in acute asthma indicates a near-fatal attack and indicates the need for consideration of intensive care admission and ventilation.229 The trial of Perrin et al suggests that many cases of hypercapnic respiratory failure in acute asthma may be due to excessive oxygen therapy. It remains appropriate to give oxygen to patients with acute severe asthma in the absence of oximetry or blood gas results, but there is no evidence of benefit from giving oxygen to patients who are not hypoxaemic and the above study suggests that unnecessary oxygen administration may cause harm. Oxygen should not be withheld from hypoxaemic patients with severe asthma because of concerns about possible hypercapnia, but oxygen therapy should be confined to what is necessary to achieve a saturation range of 94–98%.266 ,267
Evidence statements
▸ Patients with acute asthma should not be given high-concentration oxygen therapy in the absence of severe hypoxaemia (evidence level 4).
▸ The suggested target saturation range of 94–98% in acute asthma is based on expert opinion in the absence of randomised trials (evidence level 4).
Recommendation
F1: In acute asthma, aim at an oxygen saturation of 94–98% (see tables 2 and 3 and sections 8.11 and 8.13) (grade D).
The BTS guideline for pneumonia recommends aiming at an oxygen saturation target range of 94–98% in uncomplicated pneumonia with appropriate adjustments for patients with COPD, guided by blood gas measurements.268 The present guideline endorses these principles. It has recently been demonstrated that high-concentration oxygen therapy can increase transcutaneous CO2 level in patients presenting with suspected community-acquired pneumonia.137
Evidence statement
The use of oxygen in pneumonia is based on expert opinion (evidence level 4).
Recommendation
F2: In cases of pneumonia who are not at risk of hypercapnic respiratory failure, aim at an oxygen saturation of 94–98% (grade D).
Most patients with cancer who present with acute breathlessness have a specific causative factor such as a pleural effusion, pneumonia, COPD, anaemia or collapse of a lobe or collapse of a whole lung.269 ,270 Relief of breathlessness may be achieved by treating these causative factors or by the use of opioid medicines but there is increasing evidence that supplemental oxygen does not relieve breathlessness for non-hypoxaemic patients with cancer, as discussed in section 8.17. However, it is likely that patients with cancer with significant hypoxaemia may have some relief from breathlessness if given oxygen.
Evidence statement
The use of oxygen in the acute management of lung cancer is based on expert opinion and extrapolation from observational studies (see separate advice on palliative care in section 8.17; evidence level 4).
Recommendation
F3: In acute breathlessness due to lung cancer, aim at an oxygen saturation of 94–98% unless there is coexisting COPD. See also ‘Oxygen use in palliative care’ section 8.17 (grade D).
It is recognised that patients with fibrosing lung conditions such as idiopathic pulmonary fibrosis may have acute deteriorations or exacerbations, often during intercurrent chest infections. Other patients may present acutely with breathlessness due to extrinsic allergic alveolitis, sarcoidosis or other types of parenchymal lung disorders. These patients often have a high degree of V/Q mismatch and a requirement for high oxygen concentrations to achieve satisfactory blood gases and they are not at risk of hypercapnia. The oxygen level should be adjusted to maintain an oxygen saturation in the range of 94–98%, but this level may not be achievable or only achievable with a reservoir mask. Patients with severe idiopathic pulmonary fibrosis are rarely suitable for invasive ventilation or NIV because of the progressive nature of the condition.
Evidence statement
The use of oxygen in deteriorating pulmonary fibrosis is based on expert opinion (evidence level 4).
Recommendation
F4: In acute deterioration of pulmonary fibrosis or other interstitial lung diseases, aim at an oxygen saturation of 94–98% or the highest possible if these targets cannot be achieved (grade D).
As with pleural effusions, patients with a large pneumothorax may be breathless and hypoxaemic and may require supplemental oxygen for symptom relief pending definitive treatment by aspiration or drainage. However, high-concentration inhaled oxygen can also increase the rate of reabsorption of air from a pneumothorax up to fourfold.271 A 2012 study using rabbits with traumatic pneumothorax confirmed that resolution time was significantly faster with high FiO2 but there was evidence of lung toxicity above 60% oxygen.272 The BTS guideline on the management of pneumothorax recommends the use of high-concentration oxygen (reservoir mask) in all patients without COPD who require hospital admission for observation due to a moderate-sized pneumothorax that does not require drainage.273 Once a pneumothorax is drained or aspirated successfully, the patient should not require oxygen therapy unless there is additional pathology such as pneumonia, asthma or COPD requiring specific treatment.
Evidence statement
The use of oxygen in pneumothorax is based on expert opinion and extrapolation from observational studies (evidence level 4).
Recommendations
F5: In most cases of pneumothorax, aim at an oxygen saturation of 94–98% if the patient is not at risk of hypercapnic respiratory failure (grade D).
F6: In patients with pneumothorax having hospital observation without drainage, the use of high-concentration oxygen (15 L/min flow rate via reservoir mask) is recommended unless the patient is at risk of hypercapnic respiratory failure (grade D).
If a pleural effusion is causing significant breathlessness, the most effective treatment is to drain the effusion. Hypoxaemic patients with pleural effusions are likely to benefit from supplementary oxygen therapy. The BTS guidelines for management of pleural effusions do not give any specific advice concerning oxygen therapy, but it seems reasonable to give supplementary oxygen to hypoxaemic patients to maintain a saturation of 94–98%.
Evidence statement
The use of oxygen in pleural effusion is based on expert opinion (evidence level 4).
Recommendation
F7: In pleural effusion, aim at an oxygen saturation of 94–98% (or 88–92% if the patient is at risk of hypercapnic respiratory failure) (grade D).
Most patients with suspected pulmonary embolism have normal oxygen saturation and the main focus of treatment is to reach a specific diagnosis and to start anticoagulant treatment. These patients do not require oxygen therapy unless there is hypoxaemia. In these cases, the lowest concentration of oxygen that will achieve a target saturation of 94–98% is recommended. However, patients with massive or multiple pulmonary embolism may be profoundly hypoxaemic and should initially be given high-concentration oxygen via a reservoir mask to achieve an oxygen saturation of 94–98% pending definitive treatment such as thrombolysis. It has been suggested that the blood oxygen saturation may underestimate the severity of pulmonary artery obstruction in acute pulmonary embolism if shock is present.274
Evidence statement
The use of oxygen in pulmonary embolism is based on expert opinion (evidence level 4).
Recommendation
F8: In pulmonary embolism, aim at an oxygen saturation of 94–98% (or 88–92% if the patient is at risk of hypercapnic respiratory failure) (grade D).
Most patients with acute heart failure are breathless, usually due to pulmonary oedema or low cardiac output, especially if cardiogenic shock is present. The pathophysiology of oxygen transport in cardiogenic shock has been discussed in detail by Creamer et al.275 It has been shown in an animal model that the ventilatory failure of cardiogenic shock may be due to an impairment of the contractile process of the respiratory muscles.276 Miñana et al277 did not find increased mortality in Spanish patients with acute heart failure who had hypoxaemia defined as PaO2<60 mm Hg (8 kPa) which would correspond to saturation below about 91% at normal pH. In addition to specific treatment for heart failure, patients should be given supplemental oxygen to maintain a saturation of 94–98%. This is consistent with the European Society of Cardiology Task Force and European Society of Intensive Care recommendation that patients with acute heart failure should receive oxygen to maintain SpO2 of >90%.278 Patients with marked hypoxaemia (saturation <85%) should be treated with a reservoir mask initially and patients with coexisting COPD will require a lower target saturation of 88–92% pending the availability of blood gas results.
Evidence statements
The use of oxygen in acute heart failure is based on expert and extrapolation from observational studies (evidence level 4).
In hospital settings, patients with acute pulmonary oedema may benefit from CPAP and from non-invasive ventilatory support (evidence level 1+, see evidence statement in section 8.19.2).
Recommendations
F9: In acute heart failure, aim at an oxygen saturation of 94–98% (or 88–92% if the patient is at risk of hypercapnic respiratory failure) (grade D).
F10: CPAP with entrained oxygen or high-flow humidified nasal oxygen to maintain saturation 94–98% (or 88–92% if at risk of hypercapnia) should be considered as an adjunctive treatment to improve gas exchange in patients with cardiogenic pulmonary oedema who are not responding to standard treatment (or NIV if there is coexistent hypercapnia and acidosis) (grade B).
If breathlessness is due to severe anaemia, the specific treatment is blood transfusion. Studies by Canadian researchers in the late 1990s have shown that haemoglobin levels of 70 g/L (7 g/dL) were as safe as transfusion to higher levels and may produce fewer complications in the critically ill.72 However, this study was conducted using non-leucocyte-depleted blood and it is possible that some of the complications in the group who were given more transfusions might have been avoided by the use of leucocyte-depleted blood. The optimal transfusion target for critically ill patients therefore remains the subject of ongoing discussion among experts in critical care medicine and readers are referred to national guidelines for blood transfusion.279 Giving oxygen to increase an already normal oxygen saturation will have very little effect on the oxygen-carrying power of the blood, but it is reasonable to administer supplemental oxygen to maintain a saturation of 94–98% if the saturation is below these levels breathing air or if breathlessness is a very prominent symptom.
Evidence statement
The use of oxygen in anaemia is based on expert opinion based on blood gas physiology (evidence level 4).
Recommendations
F11: In anaemia, aim at an oxygen saturation of 94–98% or 88–92% if the patient is at risk of hypercapnic respiratory failure (grade D).
Good practice point
✓ Correction of anaemia by blood transfusion should be based on national guidelines.
Patients with sickle cell disease frequently present with an acute painful crisis and less frequently with an ‘acute chest syndrome’ comprising breathlessness, chest pain and fever with pulmonary infiltrates on the chest radiograph. The exact causes and mechanisms are not well understood, but oxygen should be given to all hypoxaemic patients with sickle cell crisis to avoid further intravascular sickling. There are no randomised studies of oxygen therapy in acute chest syndrome and no randomised studies of acute painful crisis in adults, but two small randomised trials showed no clinical benefit in non-hypoxaemic children with acute painful crisis.280 ,281 Patients with sickle cell disease may have a reduced oxygen saturation even when clinically stable. Homi et al282 reported a mean saturation of only 92.5% (95% CI 92.0% to 93.0%) in a group of children and young adults (age 9–18 years) with stable sickle cell disease compared with an average saturation of 97.1% (95% CI 98.8% to 97.3%) in a local control group. The British Committee for Standards in Haematology recommended in 2003 that oxygen should be given if the oxygen saturation falls below what is normal for the individual patient or a default target of 95% if the usual saturation is unknown.283 The 2012 NICE guideline reinforced this advice.284 This is consistent with the advice in the present guideline to aim at a normal or near-normal oxygen saturation for non-hypoxaemic patients with a target saturation of 94–98%. Readers are referred to the guideline on sickle cell disease for disease-specific management of this condition.283
Evidence statement
During an acute sickle cell crisis, low SaO2 as assessed by pulse oximetry is common. Research suggests that this usually indicates a low PaO2 although during an acute painful crisis pulse oximetry may underestimate the true SaO2. Desaturations during an acute sickle cell crisis should be treated with oxygen to reduce further sickling and progression of the crisis with further vaso-occlusive events (evidence level 1−).
Recommendation
F12: In sickle cell crisis and acute chest syndrome, aim for an oxygen saturation of 94–98% or aim at the saturation level that is usual for the individual patient (grade D).
Good practice point regarding sickle cell crisis
✓ Arterial or arterialised capillary blood gases should be sampled if there is any doubt about the reliability of oximetry during a sickle cell crisis.
Tables 1–4 are based on section 8, they are shown at the front of the document (see also table 3).
COPD is the best known condition that can predispose to hypercapnic (type 2) respiratory failure with acidosis, especially if the blood oxygen level is increased above 10 kPa (75 mm Hg).43 ,45 However, there are a number of other conditions which can render patients vulnerable to hypercapnic respiratory failure. The emphasis for such patients is to avoid clinically harmful levels of hypoxaemia or hypercapnia by giving carefully titrated oxygen therapy or, if necessary, by supporting the patient with the use of non-invasive or invasive mechanical ventilation.
Patients without COPD at risk of hypercapnic respiratory failure include the following:
CF.
Non-CF bronchiectasis (often in association with COPD or severe asthma).
Severe kyphoscoliosis or severe ankylosing spondylitis.
Severe lung scarring from old tuberculosis (especially with thoracoplasty).
Morbid obesity (BMI>40 kg/m2).
Musculoskeletal disorders with respiratory muscle weakness, especially if on home ventilation.
Overdose of opioids, benzodiazepines or other respiratory depressant drugs.
There is an extensive literature documenting the effects of high-concentration oxygen therapy in acute COPD.43–45 ,48 ,85 ,87 ,103 ,114 ,117 ,130 ,285–298 These reports show that the administration of supplemental oxygen to patients with exacerbated COPD (or with severe but stable COPD) often causes a rise in PaCO2 with subsequent respiratory acidosis for reasons summarised in section 5.3. The literature up to 2001 is summarised in detail in the review by Murphy et al.84 Some patients with COPD are prone to repeated episodes of hypercapnic respiratory failure in response to oxygen therapy and others may not ever suffer from this complication. Apart from patients with recurrent hypercapnic respiratory failure, it is not possible to predict if individual patients with COPD will develop hypercapnia during an acute exacerbation, so all patients with moderate or severe COPD should be considered to be at risk of this complication until the results of blood gas measurements are available. It is therefore important that patients who are at risk of having COPD should be diagnosed accurately, and this can only be done by measurement of spirometry.1 The advice given for patients with COPD also applies to other forms of fixed airflow obstruction such as patients with chronic irreversible asthma or fixed airflow obstruction associated with bronchiectasis.
Some patients with acute severe exacerbations of COPD may be too breathless to undertake spirometry on arrival in hospital, but NICE guidance is that all patients should have the test performed before discharge from hospital to confirm the diagnosis of COPD and to assess the severity of the condition.1 There is very little literature describing the effects of oxygen therapy in the other conditions listed above, but patients with these conditions are recognised to be at risk of hypercapnic respiratory failure and should be treated in a manner analogous to patients with COPD.
It has been shown that patients with COPD with a pH reading <7.35 ([H+]>45 nmol/L) despite controlled oxygen therapy are more likely to die and more likely to meet criteria for intubation and ventilation.43 ,285 ,289 One of these reports also showed that patients with a high PaO2 on arrival in hospital (>10.0 kPa or 75 mm Hg) were more likely to meet criteria for ventilation and the severity of acidosis was related to high PaO2 values.43 Based on these results, Plant et al43 recommended an upper limit of about 92% saturation for patients with exacerbations of COPD to prevent the PaO2 rising above 10 kPa. This report was supported by the work of Joosten et al45 which showed that a PaO2 of >74.5 mm Hg (10 kPa) in acute COPD was associated with an increased likelihood of admission to a HDU, increased need for NIV and a longer stay in hospital.
Roberts et al46 reported outcomes among 5052 patients with exacerbated COPD where oxygen therapy in the ambulance was documented. They found that the mortality was 7.2% in patients who were managed with <35% oxygen but mortality was 11.1% in those given ≥35% oxygen and the need for NIV increased from 9% to 22% when high-flow oxygen was given.
Based on the above literature, this guideline recommends a maximum saturation of 92% while awaiting blood gas results in AECOPD and other conditions that may predispose to hypercapnic respiratory failure. Although the rise in PaCO2 (and fall in pH) is greatest in patients who are given sufficient oxygen therapy to elevate the PaO2 above 10 kPa, it is important to note that hypercapnia can occur in acute COPD even if the oxygen saturation is <88%.296 The best management strategy for patients with persistently acidotic COPD is a trial of NIV with supplemental oxygen therapy, if required to maintain oxygen saturations 88–92%.43 ,209 ,299
Some patients with previous hypercapnic respiratory failure will have alert cards or an entry in their electronic record to alert the emergency team to the optimal concentration of oxygen required during the patient's previous hospital admissions (see section 9.7). In the absence of such information, it is suggested that a target of 88–92% should be set initially for patients with a history of previous NIV or invasive ventilation and, if necessary, modified later based on blood gas results. These patients should be categorised as very urgent by ambulance teams and emergency services, requiring immediate blood gas measurement and senior assessment on arrival at the hospital emergency department. Against this background, the study of Austin et al51 has strengthened the advice given in this guideline. These authors randomised 405 patients with presumed exacerbation of COPD to high-concentration oxygen (8–10 L/min via reservoir mask) or to titrated oxygen treatment with target range 88–92% using nasal cannulae (with nebulised bronchodilator therapy driven by compressed air). Mortality was 9% among those given high-concentration oxygen and 4% among those randomised to targeted oxygen therapy. For patients with spirometrically confirmed COPD, mortality was 9% vs 2%, respectively. Further support for targeted oxygen therapy was supplied in the 2012 study of Cameron et al.135 They undertook retrospective review of the records of 254 COPD admissions to one hospital and they found that both hypoxaemia (PaO2<60 mm Hg or 6 kPa) and hyperoxaemia (PaO2>100 mm Hg or 13.3 kPa) were associated with increased risk of serious adverse outcome, defined as a composite of hypercapnic respiratory failure, assisted ventilation or inpatient death. Twenty-four per cent of patients were hyperoxaemic and these patients had OR of 9.2 for serious adverse outcome compared with normoxaemia. Hypoxaemia occurred in 33% of patients and was associated with an OR of 2.2 for serious adverse outcome. Expressed in terms of the BTS guideline target range, the OR for serious adverse outcome was 2.0 for those with saturation below 88% compared with 88–92%. There was no increase in risk in the range of 93–96% but the OR for serious adverse outcome was 2.4 if the saturation was above 96%. The evidence for targeted oxygen therapy in exacerbated COPD is now so strong that it is unlikely that ethical approval would be granted for any further trials that randomised patients to high-concentration oxygen. However, it is not known if 88–92% is necessarily the ideal saturation range and it would be ethical to randomise patients with COPD to targeted oxygen with a target range slightly above or below or slightly wider or narrower than 88–92%.
Unfortunately, clinical studies have shown that patients with COPD are frequently given very high concentrations of oxygen, either because of misdiagnosis or because the risks of hyperoxia in patients with COPD have been overlooked.43–45 ,285 Many patients with COPD are unaware of the diagnosis or are mislabelled as having asthma (see section 9.5). The diagnosis of COPD should be communicated clearly to the patient because ambulance teams have difficulty differentiating asthma and COPD in the prehospital setting. In a recent Australian study, only 57% of 1048 patients recorded as COPD by ambulance teams had an emergency department discharge diagnosis of COPD.300
The consensus from the literature in the past was that patients with AECOPD should be treated with Venturi masks to minimise the risks of hypercapnic respiratory failure.84 However, with the availability of continuous oximetry during medical emergencies, it is now possible to titrate the flow of oxygen from nasal cannulae to achieve the desired target range and nasal cannulae were used in the only randomised trial of targeted oxygen therapy for patients with COPD.51 If Venturi masks are used, it is not yet known if it is better to start with a 28% Venturi mask or a 24% Venturi mask. Initial management with a 28% Venturi mask appears to be safe.301 The current guideline recommends starting with either a 28% Venturi mask of 1–2 L of nasal oxygen in cases of COPD with no known history of hypercapnic respiratory failure, with downward adjustment to a 24% mask (in hospital) if the saturation rises above 92%. In cases of prior hypercapnic failure who do not have an oxygen alert card, it is recommended that prehospital treatment should be started using a 28% Venturi mask at 4 L/min or a 24% Venturi mask in hospitals (and prehospital if available) with a target saturation of 88–92%. Observational studies in the 1960s suggested that a PaO2 of 50 mm Hg or 6.7 kPa (saturation about 84%) will prevent death from hypoxaemia in acute COPD exacerbations.290 ,291 If the saturation should fall below 88% despite treatment with a 24% or 28% Venturi mask, the patient should be treated with nasal cannulae or a simple face mask with the flow adjusted to maintain a saturation of 88–92% pending the availability of blood gas results. This small subgroup of patients is at very high risk of death and should be treated as a high priority on arrival in emergency departments, requiring immediate senior assessment and ABG measurements.
Evidence statements
▸ The target saturation in patients with COPD who are at risk of hypercapnia is 88–92% (evidence level 1+).
▸ The target saturation for patients with other risk factors for hypercapnia (eg, morbid obesity, chest wall deformities or neuromuscular disorders or fixed airflow obstruction associated with bronchiectasis) is 88–92% based on expert opinion which is extrapolated from observational studies (evidence level 4).
Recommendations
G1 (also A3): For most patients with known COPD or other known risk factors for hypercapnic respiratory failure (eg, morbid obesity, CF, chest wall deformities or neuromuscular disorders or fixed airflow obstruction associated with bronchiectasis), a target saturation range of 88–92% is suggested pending the availability of blood gas results (grade A for COPD, grade D for other conditions).
G2: Some patients with COPD and other conditions are vulnerable to repeated episodes of hypercapnic respiratory failure. In these cases, it is recommended that treatment should be based on the results of previous blood gas estimations during acute exacerbations. For patients with prior hypercapnic failure (requiring NIV or intermittent positive pressure ventilation) who do not have an alert card, it is recommended that low-concentration oxygen treatment should be started using a 24% Venturi mask at 2–3 L/min (or a 28% Venturi mask at 4 L/min or nasal cannulae at 1–2 L/min if a 24% mask is not available) with an initial target saturation of 88–92% pending urgent blood gas results. these patients should be treated as a high priority by emergency services and the oxygen concentration should be reduced if the saturation exceeds 92% but increased if it falls below 88% (grade D).
Good practice points for COPD and other conditions that may cause hypercapnic respiratory failure
Diagnosis of COPD or suspected exacerbation of COPD:
If the diagnosis is unknown, patients over 50 years of age who are long-term smokers with a history of chronic breathlessness on minor exertion such as walking on level ground and no other known cause of breathlessness should be treated as having suspected COPD for the purposes of this guideline.
Spirometry should be measured at least once during hospital admissions for suspected COPD (as per NICE COPD guideline1). Measurement of spirometry may confirm (or exclude) a diagnosis of airflow obstruction and the FEV1 level is a useful indicator of disease severity in COPD.
Immediate management of patients with known or suspected COPD:
If the saturation remains below 88% in prehospital care despite a 28% Venturi mask, change to nasal cannulae at 2–6 L/min or a simple face mask at 5 L/min with target saturation of 88–92% and alert the emergency department that the patient is to be treated as a high priority.
Patients with a respiratory rate >30 breaths/min should have the flow rate from Venturi masks set above the minimum flow rate specified for the Venturi mask packaging to compensate for the patient's increased inspiratory flow (see figure 11B). Increasing the oxygen flow rate into a Venturi mask does not increase the concentration of oxygen which is delivered.
Patients with a significant likelihood of severe COPD or other illness that may cause hypercapnic respiratory failure should be triaged as very urgent on arrival in hospital emergency departments and blood gases should be measured on arrival in hospital.
Prior to availability of blood gas measurements, use a 24% Venturi mask at 2–3 L/min or nasal cannulae at 1–2 L/min or 28% Venturi mask at 4 L/min and aim for an oxygen saturation of 88–92%
Initial hospital management of patients with exacerbation of COPD:
Patients with exacerbations of COPD need careful monitoring for hypercapnic (type 2) respiratory failure with respiratory acidosis which may develop in the course of a hospital admission even if the initial blood gases were satisfactory.
Avoid excessive oxygen use in patients with COPD. The risk of respiratory acidosis in patients with hypercapnic respiratory failure is increased if the PaO2 is above 10.0 kPa due to previous excessive oxygen use.
If following blood gas measurements the pH and PCO2 are normal, aim for an oxygen saturation of 94–98% unless there is a history of previous hypercapnic respiratory failure requiring NIV or intermittent positive pressure ventilation or if the patient's usual oxygen saturation when clinically stable is below 94% (these patients should have a target range of 88–92%). Blood gases should be repeated at 30–60 min to check for rising PCO2 or falling pH.
Recheck blood gases after 30–60 min (or if there is evidence of clinical deterioration) for all patients with COPD or other risk factors for hypercapnic respiratory failure even if the initial PCO2 measurement was normal.
If the PCO2 is raised but pH is ≥7.35 ([H+]≤45 nmol/L) and/or a high bicarbonate level (>28 mmol/L), the patient has probably got long-standing hypercapnia; maintain target range of 88–92% for these patients. Blood gases should be repeated at 30–60 min to check for rising PCO2 or falling pH.
If the patient is hypercapnic (PCO2>6 kPa or 45 mm Hg) and acidotic (pH<7.35 or [H+]>45 nmol/L), start NIV with targeted oxygen therapy if respiratory acidosis persists for more than 30 min after initiation of standard medical management.
For patients using Venturi masks, consider changing from Venturi mask to nasal cannulae once the patient has stabilised.
For patients who use LTOT for severe COPD, a senior clinician should consider setting a patient-specific target range if the standard range of 88–92% would require inappropriate adjustment of the patient's usual oxygen therapy while the patient is in hospital.
Management of hypercapnia or respiratory acidosis due to excessive oxygen therapy—avoidance of life-threatening rebound hypoxaemia (see section 6.3.2)
If a patient is suspected to have hypercapnic respiratory failure due to excessive oxygen therapy, the oxygen therapy must be stepped down to the lowest level required to maintain a saturation range of 88–92%. This may be achieved using 28% or 24% oxygen from a Venturi mask or 1–2 L/min via nasal cannulae depending on oxygen saturation and subsequent blood gas measurements.
Sudden cessation of supplementary oxygen therapy can cause life-threatening rebound hypoxaemia with a rapid fall in oxygen saturations below the starting oxygen saturation prior to the start of supplementary oxygen therapy.
Patients with breathlessness due to CF should be managed in a Cystic Fibrosis Centre unless this is not possible for geographical reasons. If not possible, all cases should be discussed with the Cystic Fibrosis Centre or managed according to a protocol that has been agreed with the regional centre. Patients with advanced CF may suffer from exacerbations which are similar to exacerbations of advanced COPD with associated hypoxaemia and hypercapnia. The principles of management are similar to those in AECOPD, including a need to maintain adequate oxygen saturation and avoiding excessive hypercapnia and acidosis. As in COPD, NIV may be of value in severe cases.302 NIV in CF may also be helpful to reduce symptoms (eg, work of breathing and breathlessness) and assist in airway clearance.
It is recommended that patients with acute exacerbations of CF should be managed on similar lines to patients with AECOPD with a target oxygen saturation of 88–92% for most patients, but recognition that individual patients may need to be managed differently on the basis of previous and current blood gas measurements. One study has shown that patients with a respiratory rate above 30 breaths/min often have an inspiratory flow rate above the minimum flow rate specified on the mask packaging and may therefore benefit from a doubling of this flow rate.303 However, there is no direct experimental evidence of the clinical effectiveness of increased flow rates from Venturi devices. It is possible that patients with very high inspiratory flow rates might benefit from a 28% Venturi mask with the flow rate set at 6–8 L/min to minimise the risk of the inspiratory flow rate exceeding the gas flow rate (see section 10.2.3). Patients with CF who have had previous episodes of hypercapnic respiratory failure should be issued with an oxygen alert card with recommendations based on previous blood gas measurements.
Evidence statement
▸ The optimal oxygen saturation level for patients with acute exacerbations of CF has not yet been investigated in clinical trials. Expert opinion advises treating these patients in a similar manner to patients with AECOPD who are at risk of hypercapnic respiratory failure (evidence level 4).
Recommendation
G3: Initial oxygen treatment of CF exacerbations should be similar to the initial oxygen treatment of COPD exacerbations with target saturation 88–92% (see sections 8.12.1–8.12.2) (grade D).
Hypoxaemia due to musculoskeletal and neurological disorders may be associated with acute illness (such as a chest infection) superimposed on a chronic neuromuscular condition. However, muscle weakness can be acute, subacute (eg, Guillain-Barre’ syndrome) or chronic (see section 8.13.6). For most patients with inadequate ventilation due to neuromuscular weakness, non-invasive or invasive ventilatory support is more useful than supplementary oxygen and these patients are at risk of hypercapnic respiratory failure which may be aggravated by high concentrations of oxygen. For this reason, it is recommended that spirometry should be monitored carefully and blood gases should be obtained as early as possible in all such cases. Pending the availability of blood gas results, a saturation target of 88–92% will avoid the risks of severe hypoxaemia or severe hypercapnia. The NICE guidance on NIV in motor neurone disease is also applicable to other neuromuscular conditions causing respiratory failure.304
▸ Evidence statement
The optimal oxygen saturation level for patients with musculoskeletal and neurological disorders has not yet been investigated in clinical trials. Expert opinion advises urgent blood gas assessment and early consideration of NIV with a target saturation of 88–92% while blood gas results are awaited (evidence level 4).
Recommendation
G4: In the initial management of musculoskeletal and neurological disorders with acute respiratory failure or acute-on-chronic respiratory failure, aim at an oxygen saturation of 88–92% and measure blood gases to determine if NIV will be required (grade D).
Good practice point regarding patients with neurological disorders
Patients with respiratory failure due to neurological disorders or muscle disease are at high risk of dying and require urgent assessment to determine if they are likely to require non-invasive or invasive ventilator support rather than oxygen therapy. Monitor these patients with blood gases and regular spirometry (forced vital capacity). Patient's wishes regarding this form of treatment should be established as early as possible in the course of the illness, ideally before an acute episode has developed.
Patients with the OHS are chronically hypercapnic unless treated with NIV and may decompensate acutely resulting in hypercapnic respiratory failure with acidosis.305 One study has found the incidence of hypoventilation to be as high as 31% in a cohort of obese hospitalised patients.306 Wijesinghe et al47 have demonstrated in 2011 that breathing 100% oxygen causes worsening hypercapnia in stable patients with obesity-associated hypoventilation. For purposes of oxygen therapy, patients with morbid obesity should be treated in a similar manner to patients with an AECOPD. The target saturation will usually be 88–92% but, as with COPD, a lower target range may be appropriate for individual patients based on blood gas measurements during a previous exacerbation or due to acute acidosis. Assessment of patients with increasing shortness of breath or worsening oxygen saturation must include blood gases. As in COPD, patients with respiratory acidosis may benefit from NIV.
Evidence statement
Patients with OHS are at risk of worsening hypercapnia when administered high-flow oxygen (evidence level 1+).
However, the optimal oxygen saturation level for patients with OHS has not yet been investigated in clinical trials. Expert opinion advises treating these patients in a similar manner to patients with AECOPD who are at risk of hypercapnic respiratory failure (evidence level 4).
Recommendations
G5: Morbidly obese patients (BMI>40 kg/m2), even without evidence of coexistent OSA are at risk of hypoventilation and should be given titrated oxygen to maintain a target saturation of 88–92% (grade D).
G6: NIV should be considered for hypercapnic patients with COPD, CF, neuromuscular disorders or morbid obesity who are at risk of hypercapnic respiratory failure if the pH is <7.35 or [H+]>45 nmol/L (grade D). See BTS/ICS Guideline for the ventilatory management of acute hypercapnic respiratory failure (ref 299).
There are a number of conditions such as myocardial infarction, angina and stroke for which oxygen was traditionally given to all patients in an attempt to increase oxygen delivery to the heart or brain. However, the administration of supplemental oxygen to normoxaemic patients has very little effect on blood oxygen content but may reduce myocardial and cerebral blood flow due to vasoconstriction which is a physiological response to hypoxia in most vital organs. There is no evidence of benefit from the administration of supplemental oxygen to non-hypoxaemic patients with these conditions and there is some evidence of possible harm, especially when used at high-flow rates, so it is recommended that oxygen should only be given to patients with these conditions if hypoxaemia is present, usually due to complications such as heart failure or pneumonia. There are no published trials supporting the use of oxygen to relieve breathlessness in non-hypoxaemic patients, and there is evidence from randomised studies that oxygen does not relieve breathlessness compared with air in non-hypoxaemic patients with COPD who are breathless following exertion.146
Some patients with acute myocardial infarction have heart failure and should be treated accordingly (see section 8.11.9). Most patients with suspected or confirmed myocardial infarction are not hypoxaemic and most are not breathless. In the case of non-hypoxaemic patients, it is not known if supplementary oxygen may be beneficial by increasing the amount of oxygen delivered to the hypoxaemic area of myocardium or whether it may actually cause vasoconstriction with increased systemic vascular resistance and reduced myocardial oxygen supply with worsened systolic myocardial performance.307–315 A study of patients having coronary arteriography found that breathing 100% oxygen reduced coronary blood flow velocity by 20% and increased coronary resistance by 23%.316 A study of 16 healthy individuals using MRI found that coronary artery oxygen delivery fell by 11% due to decreased cardiac output and decreased left ventricular perfusion while breathing oxygen at 8 L/min via a mask despite the increased blood oxygen content.317 However, Ranchord et al318 found that high-concentration oxygen increased the time to onset of exercise-induced myocardial ischaemia in patients with stable ischaemic heart disease, suggesting that the physiology of oxygen delivery to the heart may be different during exercise in ischaemic heart disease. Reduced myocardial oxygen consumption might also be associated with reduced contractility.
There is a theoretical possibility that high oxygen levels might exacerbate reperfusion injury to the heart.314 Despite a multitude of large studies of intervention in myocardial infarction, there had been only three published randomised studies of oxygen therapy prior to 2015. A randomised trial in 1976 did not identify any benefit from such therapy but found some evidence of potential harm.319 This trial reported a significantly greater rise in aspartate aminotransferase and heart rate which could suggest increased infarct size in the oxygen treated group. There was a difference in mortality between the two groups that did not reach statistical significance (3 deaths in 77 patients treated with air vs 9 deaths in 80 patients given oxygen at 6 L/min via a simple face mask for 24 hours). This study was undertaken at a time before angiographic interventions were possible for myocardial infarction.
Ranchord et al320 randomised 136 patients with ST-elevation myocardial infarction to 6 L of oxygen via simple face mask or titrated oxygen to achieve saturation of 93–96% for 6 hours after randomisation in a hospital setting. The trial was conducted between 2007 and 2009 and most patients had angiographic interventions. There was no difference in troponin T level between the groups and the number of deaths was too low (3) to permit meaningful analysis. Eighty-five per cent of patients in both groups had received oxygen in the ambulance and/or emergency department for a mean of 62 min prior to randomisation and almost all patients received thrombolysis or percutaneous coronary intervention within 4 hours of onset of chest pain. Therefore, this study really evaluated the effect of stopping oxygen therapy prior to therapeutic intervention in a group of patients of whom most had already received oxygen for more than 1 hour.
The third study was an open-label randomised study conducted in Russia which was reported with limited methodological details.321 Twenty-eight patients received oxygen in addition to standard therapy for 30 min prior to myocardial revascularisation and for 3 hours after the intervention, 30 patients received oxygen for 3 hours after the intervention and 79 patients received ‘standard therapy’. Details of oxygen therapy prior to randomisation were not given. This study reported one death among 58 patients randomised to oxygen therapy and no deaths among 79 patients randomised to standard therapy but the authors reported fewer complications among those randomised to oxygen.
A systematic review and a historical review of oxygen therapy in acute myocardial ischaemia have both concluded that there was no evidence to support this practice in non-hypoxaemic patients and some evidence of possible harm.322 ,323 Further systematic reviews and meta-analysis in 2011 and 2012 concluded that the existing studies lacked power, no clear conclusions can be drawn and further studies are needed.324 ,325 One study from 1969 showed that hypoxaemia did not affect the availability of oxygen for myocardial metabolism in normal participants until the oxygen saturation fell to about 50%, but evidence of myocardial ischaemia was seen at saturations of 70–85% in participants with coronary artery disease.326 In these circumstances, it is advised that patients with myocardial infarction or chest pain suspicious of myocardial infarction should be given supplementary oxygen if required to maintain a saturation of 94–98%.
The study by Wilson and Channer4 in 1997 showed that desaturation below 90% was common in patients with myocardial infarction within the first 24 hours of admission to a coronary care unit, but these authors may not have been aware that nocturnal desaturation to this level is very common in healthy individuals.33 Wilson and Channer4 did not demonstrate any correlation between hypoxaemic events and adverse cardiac events. They did, however, show that monitoring by oximetry was inadequate in UK coronary care units in the mid-1990s.
The 2010 NICE Guideline for Chest Pain of recent onset recommends setting an oxygen target saturation range of 94–98% based on the arguments discussed above and the advice given in the 2008 BTS Emergency Oxygen Guideline.327 The 2012 guidelines for acute myocardial infarction of the European Society for Cardiology recommends the following: “Oxygen (by mask or nasal prongs) should be administered to those who are breathless, hypoxic (SaO2<95%), or who have heart failure.”328 The 2011 American College of Cardiology/American Heart Association guideline for Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction gives the following advice:329 “Supplemental oxygen should be administered to patients with UA/NSTEMI with an arterial saturation <90%, respiratory distress, or other high-risk features for hypoxemia.” This is followed by the following unreferenced advice: “It is reasonable to administer supplemental oxygen to all patients with UA/NSTEMI during the first 6 h after presentation.” The limited available evidence supports the suggestion that clinicians should aim at normal or near-normal oxygen saturation in patients with myocardial infarction, acute coronary syndrome and chest pain suspicious of coronary artery disease. A target saturation range of 94–98% will meet all of these goals, and further research of this topic should be prioritised because this is such a common medical problem and there is so little existing evidence.
Fortunately, there is one recent published study and other forthcoming studies of oxygen use for myocardial infarction in ambulances. The AVOID study in Australia was study was designed to determine whether withholding routine supplemental oxygen therapy in patients with acute ST-elevation myocardial infarction but without hypoxaemia prior to reperfusion decreases myocardial infarct size.330–332 The results have suggested that cardiac enzyme levels were higher and infarct size at 6 months was 55% bigger as determined by cardiac MR scan when oxygen was administered. Mean peak troponin was similar in the oxygen and no oxygen groups (57.4 vs 48.0 μg/L; ratio 1.20; 95% CI 0.92 to 1.56; p=0.18). There was a significant increase in mean peak creatine kinase in the oxygen group compared with the no oxygen group (1948 vs 1543 U/L; means ratio 1.27; 95% CI 1.04 to 1.52; p=0.01). There was an increase in the rate of recurrent myocardial infarction in the oxygen group compared with the no oxygen group (5.5% vs 0.9%; p=0.006) and an increase in frequency of cardiac arrhythmia (40.4% vs 31.4%; p=0.05). At 6 months, the oxygen group had an increase in myocardial infarct size on cardiac MR (n=139; 20.3 vs 13.1 g; p=0.04).331 A subsequent publication by these authors showed that there was a significant increase in troponin and creatine kinase levels which was dependent on the total dose of supplemental oxygen (litres of supplemental oxygen received) and a typical patient receiving supplemental oxygen in the first 12 hours after ST-elevation myocardial infarction would experience an ∼20% increase in myocardial infarct size.332
The DETO2X-AMI trial is a further randomised trial of oxygen versus air in the management of suspected myocardial infarction and was started in Sweden and will hopefully provide more useful information concerning the management of this common medical emergency.333
In the past, most emergency calls to ambulance services because of chest pain were treated with high-concentration oxygen in accordance with the Joint Royal Colleges Ambulance Liaison Committee (JRCALC) older guidance.334 However, this guidance was updated in 2009 to reflect the advice given in the 2008 BTS Emergency Oxygen Guideline with a target saturation range of 94–98% for most patients with chest pain.12 Most such patients have a final diagnosis of undifferentiated chest pain rather than acute coronary artery syndrome and most patients with undifferentiated chest pain are normoxaemic. The clinical management of a very large number of patients was therefore changed following the introduction of the 2008 BTS guideline and subsequent publications have tended to support the concept of aiming for normoxaemia in patients with suspected myocardial infarction.
Evidence statements
▸ The optimal oxygen saturation level for patients with myocardial infarction and acute coronary syndromes has not yet been investigated in clinical trials. Expert opinion advises maintaining normal or near-normal saturation unless the patient is at risk of hypercapnic respiratory failure (evidence level 4).
▸ There is evidence from two randomised studies that the administration of oxygen to non-hypoxaemic patients in the immediate management of myocardial infarction may be associated with increased infarct size (evidence level 1+).
Recommendation
F13: In myocardial infarction and acute coronary syndromes, aim at an oxygen saturation of 94–98% or 88–92% if the patient is at risk of hypercapnic respiratory failure (grade D).
In the past, it was customary to give supplemental oxygen to all patients with stroke to try to improve cerebral oxygenation. There are four published randomised trials of oxygen therapy in patients with stroke with normal oxygen saturation, none of which have shown benefits. A study of supplemental oxygen (2 or 3 L/min dependent on baseline oxygen saturation) for 24 hours (n=550) found no difference in 1-year survival for the entire cohort of patients with stroke and no difference in survival for patients with more severe strokes. However, a post hoc subgroup analysis found that for patients with minor strokes, 1-year mortality was 18% in the group given oxygen and 9% in the group given air (OR 0.45; 95% CI 0.23 to 0.90; p=0.02).335 A pilot study of oxygen supplementation at a rate of 2 or 3 L/min, dependent on baseline oxygen saturation for 72 hours in the UK (n=300) suggested better neurological recovery at 1 week, but showed no difference in survival and recovery at 6 months.336 ,337 The study did not find an excess risk for minor strokes in patients given oxygen. A much larger study (n=8003) using the same dose and duration of oxygen treatment has just closed and is only available in abstract format so far, but confirms that routine oxygen treatment does not reduce mortality or improve recovery.338
A small randomised trial of high-concentration oxygen therapy (10 L/min) in non-hypoxaemic patients (n=40) showed no clinical benefit339 and a study of very high-flow oxygen (45 L/min) was terminated in 2009 after enrolling 85 patients because of excess mortality in the hyperoxaemia group (40% vs 17%), the full report had not yet been published when this guideline was prepared.340 Finally, an observational study reported increased mortality associated with hyperoxaemia in ventilated patients with stroke on ICUs.341
Post-stroke hypoxaemia is common and associated with worse outcome in some small studies.342 ,343 The risk of hypoxaemia is particularly high at night, during interward transfers and in the CT scanner.342 ,344 Regular monitoring of oxygen saturation and treatment of all episodes of hypoxaemia has been shown to improve outcome in an observational study.343 It is therefore recommended to monitor oxygen saturation regularly (at least every 4 hours, including the night) during the acute phase of stroke and to treat every episode of hypoxaemia.
The most common causes of hypoxaemia after stroke are obstruction of airflow by secretions in the upper airway or complications of the stroke such as pneumonia, pulmonary embolism or heart failure. These must be addressed in every patient who develops hypoxaemia post-stroke.
It is recommended that patients with stroke should receive supplemental oxygen only after the airway has been cleared and if this treatment is required to achieve an oxygen saturation of 94–98% (88–92% for patients with coexisting risk of COPD or other risk of respiratory acidosis). High concentrations of oxygen should be avoided unless required to correct hypoxaemia. As patients with stroke tolerate nasal cannulae better than oxygen masks, oxygen should be given via nasal cannulae unless a strictly controlled oxygen concentration is indicated.345 ,346
There has also been some discussion concerning the optimal body position for the management of patients with stroke and potential hypoxaemia. A systematic review of clinical studies in conscious patients concluded that there was limited evidence that sitting in a chair had a beneficial effect and lying positions had a deleterious effect on oxygen saturation in patients with acute stroke with respiratory comorbidities, but patients with acute stroke without respiratory comorbidities can adopt any body position.161 The authors of this review recommended that people with acute stroke and respiratory comorbidities should be positioned as upright as possible as discussed in section 6 and recommendation A5. No trials have expressly addressed the best position in unconscious and semiconscious patients with stroke. As in other patient groups with a reduced level of consciousness the recovery position is recommended to safeguard the airway.
Evidence statements
High concentrations of oxygen in normoxaemic patients with stroke may be associated with increased mortality (evidence level 1−).
Routine oxygen for non-hypoxic patients with stroke does not improve recovery or reduce disability (evidence level 1−).
Patient positioning has not been shown to affect SaO2 as measured by pulse oximetry in patients without cardiorespiratory comorbidities, but sitting out in a chair improves oxygenation in patients with pre-existing cardiorespiratory disease (evidence level 1−).
Recommendation
F14: High concentrations of oxygen should be avoided in patients with stroke, unless required to maintain normal oxygen saturation. Aim at an oxygen saturation of 94–98% or 88–92% if the patient is at risk of hypercapnic respiratory failure (grade D).
Good practice points regarding stroke management
Oxygen saturation should be monitored at least every 4 hours throughout the day and night in patients with acute stroke and all episodes of hypoxaemia treated.
Patients with hypoxaemia post-stroke require medical review to establish and treat the cause.
Oxygen should only be given once the airway has been cleared and at the lowest concentration necessary to achieve an oxygen saturation of 94–98% or 88–92% if the patient is at risk of hypercapnic respiratory failure.
Oxygen should be given via nasal cannulae, unless there are clear indications for a different oxygen delivery system.
Patients with stroke and cardiorespiratory comorbidities should be positioned as upright as possible, in a chair if possible (see recommendation A5).
Patients with a reduced level of consciousness after stroke should be nursed in the recovery position with the paralysed side lowest.
Many patients who present to hospital with breathlessness are found to have no cardiopulmonary problems and many such patients have a specific diagnosis of hyperventilation, dysfunctional breathing, vocal cord dysfunction or panic attacks, sometimes in addition to asthma or some other underlying respiratory disorder.347 Many such patients will have an abnormally high oxygen saturation of 99% or 100% and clearly do not require supplemental oxygen therapy but some patients with vocal cord dysfunction may develop respiratory failure due to upper airway obstruction. Many other non-hypoxaemic patients will present to hospital with acute breathlessness of unknown cause, and the majority of patients with an elevated respiratory rate are likely to have an organic illness. In some cases, simple investigations will reveal a specific diagnosis such as pneumothorax or pneumonia or pulmonary embolism, but many cases remain undiagnosed. A policy of giving supplemental oxygen if the saturation falls below 94% will avoid exposing patients with undiagnosed medical illnesses to the risk of hypoxaemia while avoiding the unnecessary use of oxygen in patients with behavioural or dysfunctional breathlessness.
Studies in normal volunteers have demonstrated that compensatory desaturation may occur shortly after voluntary hyperventilation.348 The mean PaO2 of 10 male volunteers increased from 13.7 kPa (103 mm Hg) to 18.6 kPa (140 mm Hg) during hyperventilation but fell to a nadir of 7.8 kPa (58 mm Hg) about 7 min after cessation of hyperventilation and did not normalise until after a total of 17 min of observation. It is not known whether or not this occurs after pathological hyperventilation, but this phenomenon could cause considerable confusion if it should occur in an emergency department.
A traditional treatment for hyperventilation was to ask the participant to rebreathe from a paper bag to allow the carbon dioxide level in the blood to normalise. However, it has been shown that this practice can cause hypoxaemia with potentially fatal consequences.349 The average fall in PO2 during rebreathing was 26 mm Hg (3.5 kPa) and the maximum fall was 42 mm Hg (5.6 kPa). This guideline does not recommend rebreathing from a paper bag in cases of hyperventilation.
Good practice points regarding patients with suspected hyperventilation
Organic illness must be excluded before making a diagnosis of hyperventilation.
Patients with a definite diagnosis of hyperventilation should have their oxygen saturation monitored. Those with normal or high SpO2 do not require oxygen therapy.
Rebreathing from a paper bag can be dangerous and is NOT advised as a treatment for hyperventilation.
Many poisons and drugs can cause respiratory or cardiac depression or direct toxic effects on the lungs. The treatment of individual toxic agents is beyond the scope of this guideline. Specific antidotes such as naloxone for opioids or flumazenil for benzodiazepines should be given if available and oxygen saturation should be monitored closely. Supplemental oxygen should be given to achieve a target saturation of 94–98% pending the results of blood gas analysis (88–92% if at risk of hypercapnic respiratory failure, including patients with overdoses of narcotic agents). All potentially serious cases of poisoning should be monitored in a level 2 or 3 environment (HDU or ICU).
Three specific types of lung injury deserve special mention. Oxygen is known to be hazardous to patients with paraquat poisoning,125 ,126 and oxygen potentiates bleomycin lung injury. Because of these risks, oxygen should be given to patients with these conditions only if the oxygen saturation falls below 85%. Some authors have suggested the use of hypoxic ventilation with 14% oxygen as a specific treatment for paraquat poisoning.350 Bleomycin lung injury can be potentiated by high-concentration oxygen therapy, even if given several years after the initial lung injury.127 It is therefore recommended that high concentrations of oxygen should be avoided in patients with possible bleomycin-induced lung injury and a lower oxygen saturation target range should be accepted (eg, 88–92%).
There is evidence from animal experiments that oxygen may potentiate lung injury from aspiration of acids.128 ,129 The effect in humans is not known so patients with acid inhalation should have the usual adult target saturation range of 94–98%, but it would appear prudent to aim in the lower half of the target range for these patients and clinical trials in humans are clearly required.
Evidence statement
For most types of poisoning, the optimal oxygen saturation level has not yet been investigated in clinical trials. Expert opinion advises maintaining normal or near-normal saturation unless the patient is at risk of hypercapnic respiratory failure or unless they require high oxygen levels (carbon monoxide or cyanide poisoning) or have ingested a poison such as paraquat or bleomycin where supplemental oxygen may aggravate tissue damage (evidence level 4).
Recommendations
F15: In most poisonings, aim at an oxygen saturation of 94–98% unless the patient is at risk of hypercapnic respiratory failure (grade D).
F16: In poisoning by paraquat and poisoning by bleomycin, give oxygen only if the saturation falls below 85% and reduce or stop oxygen therapy if the saturation rises above 88% (grade D).
Many metabolic and renal disorders can cause metabolic acidosis which increases respiratory drive as the body tries to correct the acidosis by increased excretion of carbon dioxide via the lungs. Although these patients have tachypnoea, they do not usually complain of breathlessness and most have high oxygen saturation (unless there is a coexisting pulmonary or cardiac problem). Supplementary oxygen is not required for such patients unless the oxygen saturation is reduced. In such cases, oxygen should be given to maintain a saturation of 94–98%.
Evidence statement
The optimal oxygen saturation level for patients with most metabolic, endocrine and renal disorders has not yet been investigated in clinical trials. Expert opinion advises maintaining normal or near-normal saturation unless the patient is at risk of hypercapnic respiratory failure (evidence level 4).
Recommendation
F17: In most metabolic and renal disorders, aim at an oxygen saturation of 94–98% unless the patient is at risk of hypercapnic respiratory failure (grade D).
Patients with acute or subacute conditions affecting the respiratory muscles (often superimposed on chronic conditions) are at risk of sudden onset of respiratory failure with hypoxaemia and hypercapnia and may require non-invasive or invasive ventilatory support. This applies especially to patients with Guillain-Barre’ syndrome for whom spirometry (forced vital capacity) should be monitored carefully as this should detect the onset of severe respiratory failure prior to the development of hypoxaemia. If the oxygen level falls below the target saturation, urgent blood gas measurements should be undertaken and the patient is likely to need ventilatory support.
Good practice point
Patients with respiratory failure due to neurological disorders or muscle disease are at high risk of dying and require urgent assessment to determine if they are likely to require non-invasive or invasive ventilator support rather than oxygen therapy. Monitor these patients with blood gases and regular spirometry (forced vital capacity). Patient's wishes regarding this form of treatment should be established as early as possible in the course of the illness, ideally before an acute episode has developed.
Relief from cluster headache has been reported in 56–85% of cases.351–354 Benefit has recently been reported for other types of headache.355 Although this could be considered as a form of emergency oxygen therapy, these patients are not breathless or hypoxaemic. Cluster headache is one of the most severe pain disorders known to humans. Patients can attend emergency departments in an acute cluster attack but because of the relatively short duration and frequency of the episodes, home treatment of the acute cluster attack is most often undertaken. For patients with cluster headache arrangements for home and ambulatory oxygen is recommended for treatment of the acute cluster headache bout. Oxygen at a flow rate of at least 12 L/min from a reservoir mask is recommended.353 Patients who have episodic cluster headache may not need oxygen on a longer term basis and once they have been cluster headache free for over 4 weeks the oxygen supply can be uplifted. However, because of the recurrent nature of the condition, emergency supply of oxygen should be made available for cluster headache sufferers. In a study comparing the use of oxygen with air, 78% patients given oxygen at 12 L/min via reservoir mask for 15 min had a reduction in pain at 15 min as compared with 20% for those breathing air at 12 L/min (p<0.001).354 In a further study, there was a complete or substantial reduction in pain at 30 min in 56% of patients (nine participants) in 80% or more of their cluster headaches when given oxygen at 6 L/min for up to 15 min from a reservoir mask compared with 7% on air.352
Evidence statement
Oxygen therapy can provide relief from cluster headache (evidence level 1−).
Recommendation
F18: For patients with cluster headaches, oxygen should be administered using a flow of at least 12 L/min from a reservoir mask and home oxygen should be provided (grade D).
The use of oxygen has been recommended during many obstetric emergencies and, in particular, for collapse related to haemorrhage, pulmonary embolism, eclampsia or amniotic fluid embolism. Severe pre-eclampsia and eclampsia may occasionally present with pulmonary oedema and this can occur in the antenatal or postnatal periods. Medical problems such as pneumonia or acute exacerbations of asthma are not uncommon during pregnancy. Peripartum cardiomyopathy is rare but may present with heart failure in the postnatal period. Major trauma is increasingly common, particularly related to road traffic accidents.
The use of oxygen during pregnancy should follow the same general principles as the use of oxygen for other patients. Pregnant women suffering major trauma or severe hypoxaemia should be started on high-concentration oxygen via a non-rebreathing reservoir mask and those with milder hypoxaemia can use nasal cannulae or a simple face mask or Venturi mask to achieve an oxygen saturation of 94–98% in most cases. Risk factors for hypercapnia are uncommon among women of child-bearing age but morbid obesity is an increasing problem in the UK population and is associated with risk of hypercapnia (see section 8.12.4). Morbidly obese pregnant women with hypoxaemia are at risk of hypercapnia and should have a target range of 88–92% pending availability of blood gas results. Pregnant women who are fully conscious with no cardiovascular compromise may be managed in the sitting position or if lying down should use the full left lateral position. If an undelivered woman is hypoxaemic with reduced consciousness level or needing respiratory or cardiovascular support or CPR, she should be managed with left lateral tilt applied. This will improve cardiac output and may also facilitate breathing for mechanical reasons. As an alternative, the patient can be left lying relatively flat and the uterus can be displaced manually (preferably to the left) in order to relieve aortocaval compression. This will usually require additional help and is uncomfortable.
Oxygen was commonly given as part of the treatment for many obstetric emergencies. However, it is recommended that, when oxygen is administered during pregnancy or labour, clinicians should aim to achieve normoxaemia (saturation 94–98%). There is no randomised trial evidence to suggest that maternal ‘hyperoxaemia’ is beneficial to mother or fetus. A 2008 review of the use of oxygen during intrauterine resuscitation concluded as follows: “Caution should be exercised when considering maternal oxygen administration as a first-line intrauterine resuscitation measure until more data are available, reserving its use after other measures have been unsuccessful in resolving the non-reassuring fetal heart rate pattern.”356
Oxygen is often given for short periods when acute fetal compromise is suspected in labour in the hope of increasing oxygen delivery to the fetus. A Cochrane review found no trials addressing the use of oxygen for fetal compromise but the authors identified two trials of prophylactic oxygen in labour which reported a statistically significant increase in the incidence of cord blood acidosis (pH<7.20 or [H+]>63 nmol/L) in the oxygenation group (relative risk (RR) 3.5, 95% CI 1.34 to 9.19).357 A small (n=56) randomised trial in Washington, USA reported in 2012 that the delivery room resuscitation rate was 20% for infants of mothers randomised to 2 L of nasal oxygen for at least 30 min before delivery compared with 0% in those receiving air from a nasal cannula (p=0.03).358 This study reported cord blood acidosis in just one participant in each group. When this study is added to the Cochrane review, the reported prevalence of cord blood acidosis in three published studies was 18/151 (12%) in those randomised to oxygen therapy and 6/140 (4%) when air was used throughout labour. A recent clinical opinion paper included a review of the two randomised trials assessing use of maternal oxygen supplementation in labour.359 These authors also noted an absence of data confirming fetal benefit and the possibility that increased free radical activity may be harmful. The authors of this 2014 paper conclude that appropriately powered randomised trials are still required. Until then, oxygen supplementation should be reserved for confirmed maternal hypoxaemia in labour, and should not be considered an appropriate intervention for non-reassuring fetal status.
This fits with the recommendation that pregnant women with evidence of hypoxaemia should have their blood oxygen saturation maintained in the normal range (94–98%) using supplemental oxygen only when required to achieve this effect. This applies before or during labour as well as in the immediate postnatal period. The causes of maternal hypoxaemia may include trauma, pre-existing or new medical conditions as well as pregnancy-specific complications. In all of these situations the aim should be normoxaemia (saturation 94–98%).
A Cochrane review of the use of supplemental oxygen for caesarean section during regional analgesia concluded as follows: “Current evidence suggests that supplementary oxygen given to healthy term pregnant women during elective caesarean section under regional anaesthesia is associated with higher maternal and neonatal oxygen levels (maternal SpO2, PaO2, UaPO2 and UvPO2) and higher levels of oxygen free radicals. However, the intervention was neither beneficial nor harmful to the neonate's short-term clinical outcome as assessed by Apgar scores.”360
A randomised trial of postpartum oxygen inhalation concluded that this practice is not beneficial for reducing vaginal blood loss during the third and fourth stages of labour.361
Evidence statements
▸ There have been no trials comparing different oxygen regimens in acutely unwell pregnant women so management should be based on the oxygen levels that are believed to be optimal in other groups of acutely unwell adults (evidence level 4).
▸ When women in late pregnancy (ie, above 20 weeks) lie flat on their backs, aortocaval compression by the gravid uterus reduces maternal cardiac output. This is improved by using left lateral tilt or manual displacement of the uterus. Placing the patient in the full left lateral position is another alternative (evidence level 3).
▸ Although maternal oxygen therapy can increase fetal oxygen levels, there are limited data regarding its risks or possible benefits to the mother, fetus and newborn (evidence level 4)
Recommendations
H1: Women who suffer from major trauma, sepsis or acute illness during pregnancy should receive the same oxygen therapy as any other seriously ill patients, with a target oxygen saturation of 94–98%. The same target range should be applied to women with hypoxaemia due to acute complications of pregnancy (eg, collapse related to amniotic fluid embolus, eclampsia or antepartum or postpartum haemorrhage) (grade D).
H2: Women with underlying hypoxaemic conditions (eg, heart failure) should be given supplemental oxygen during labour to achieve an oxygen saturation of 94–98% unless they are at risk of hypercapnic respiratory failure (target range 88–92%) (grade D).
H3: Pregnant women who are fully conscious with no cardiovascular compromise may be managed in the sitting position or if lying down should use the full left lateral position (grade D).
H4: Pregnant women above 20 weeks gestation (uterine fundus at or above the level of the umbilicus) who are at risk of developing associated cardiovascular compromise (eg, trauma, vaginal bleeding, etc) should be positioned to avoid aortocaval compression by using left lateral tilt, manual uterine displacement or by placing them in a full left lateral position (grade D).
H5: Women who are more than 20 weeks pregnant with evidence of hypoxaemia associated with reduced consciousness or those requiring respiratory or cardiovascular support or CPR should be managed with left lateral tilt or manual uterine displacement (ideally to the left) to improve cardiac output and oxygen delivery (grade D).
H6: The use of oxygen supplementation during intrauterine fetal resuscitation during labour was widespread in the past but there is no evidence of benefit. There is weak evidence of harm to the fetus if supplemental oxygen is given for long periods during uncomplicated labour. Overall, the use of oxygen during labour is only required when there is evidence of maternal hypoxaemia (oxygen saturation <94%) (grade D).
Postoperative breathlessness and hypoxaemia can develop due to a variety of complications including atelectasis, pneumonia and pulmonary embolism. The use of opioid analgesia commonly used for moderate-to-severe pain can lead to and exacerbate respiratory failure, which can potentially be life-threatening. Historically, it has been common practice for postoperative patients to receive routine supplemental oxygen for a period ranging from hours to days after surgery to prevent hypoxaemia, particularly those receiving opioid analgesia. High-risk patients undergoing major surgery are best managed in an ICU and HDU settings which facilitate the continuous monitoring of SpO2 and usually end tidal CO2 (this is standard in ventilated patients). Regular ABG analysis using arterial lines is also available in ICU and HDU settings. This allows oxygen therapy to be administered in a dose sufficient to relieve hypoxaemia without causing hyperoxia.
However, the majority of postoperative patients are managed on general surgical wards where continuous monitoring is not possible. The question of whether all postoperative patients should receive supplemental oxygen routinely is debatable and there is lack of robust evidence from RCTs to either support or refute its use.
A number of observational studies have documented a high incidence of postoperative hypoxaemia.182 ,362–364 A Cochrane review of 22 992 patients reported on the incidence of hypoxaemia in the perioperative and postoperative period.181 Unsurprisingly, it is difficult to draw any conclusions on the overall incidence of hypoxaemia due to the variation in population groups, operative procedure and anaesthetic modality.
This same Cochrane review included data from five trials in which patients were randomised to pulse oximetry monitoring or no pulse oximetry during and after surgery.181 The review showed that pulse oximetry leads to a 1.5-fold to 3-fold reduction in perioperative hypoxaemia. However, while pulse oximetry led to the detection of hypoxaemia and interventions to correct it, there was no difference in complication rates between the two groups. Additionally postoperative cognitive function, length of hospital stay and mortality was the same in both groups. The authors suggested that correcting modest hypoxaemia, by increasing the blood oxygen saturation from marginal to satisfactory may confer no benefit to the patient. However, only small numbers of studies were included and further work is required for clarification.
The incidence of postoperative hypoxaemia demonstrated in randomised trials is again, variable. Gift et al366 found no clinically significant difference in SpO2 in nearly 300 postoperative patients randomised to four different treatments including oxygen 4 L/min via nasal cannulae, 40% oxygen via mask, nurse-led hyperinflation and no treatment.365 Canet et al365 found that the incidence of hypoxaemia was higher after breathing air compared with 35% oxygen and the incidence increased if the patients were older or if they received general anaesthesia.366
Given the potential to develop hypoxaemia and the inability to continuously monitor oxygenation in most postoperative patients, is it safer to routinely administer supplemental oxygen to all patients to prevent hypoxaemia? The major disadvantage to this approach is that while supplemental oxygen will correct hypoxaemia it can mask the ability to detect hypoventilation.228 Additionally, recently, Niesters et al107 have shown that hyperoxia has an additive effect on opioid-induced respiratory depression. Furthermore, there is a large body of evidence showing hyperoxia is associated with haemodynamic alterations which may increase myocardial ischaemia and impair cardiac performance (see section 8.13.1). A recent randomised trial of 340 patients postcardiac surgery administering nasal high-flow oxygen compared with usual care (oxygen to keep SpO2>93%) showed no improvement in postoperative oxygenation.367 However, patients in the high-flow group were less likely to require escalation of respiratory support at any time during the study (47 patients in the high-flow group (27.8%) compared with 77 patients (45%) in the standard care group (OR 0.47, 95% CI 0.29 to 0.7, p<0.001). The authors hypothesised that the low-level airway pressure support provided by the nasal high-flow system may have influenced this outcome.
In a recent editorial, Martin and Grocott368 highlight the need to re-evaluate the unrestricted use of oxygen by anaesthetists. They discuss the relationship between oxygen therapy in perioperative care, critical care and resuscitation, highlighting the lack of clinical benefit from hyperoxaemia and the potential to lead to poor outcomes. They propose a strategy of ‘precise control of arterial oxygenation’ in which oxygen is administered to a defined target, for example, PaO2 of 8–10 kPa or SaO2 88–92% thus avoiding potential harm from hypoxaemia and hyperoxaemia and improving clinical outcomes. These recommendations are in keeping with this present guideline.
The ‘routine’ use of supplemental oxygen postoperatively, therefore remains controversial.76 ,181 ,369–372 More evidence from RCTs is required. Regular, but not necessarily, continuous oxygen saturation monitoring is mandatory. In keeping with the 2004 SIGN guideline on postoperative care which recommends maintaining an oxygen saturation above 92% for postoperative patients, this present guideline recommends administering oxygen to maintain a target saturation of 94–98% for most patients, and a target saturation of 88–92% in those patients at risk of hypercapnic respiratory failure.370
Evidence statement
Pulse oximetry in the perioperative period leads to a significant reduction in perioperative hypoxaemia. However, identification and correction of mild or moderate hypoxaemia with pulse oximetry does not lead to a reduction in complication rates, length of stay or mortality (evidence level 1+).
Good practice points
A target saturation of 94–98% is recommended for most surgical patients except those at risk of hypercapnic respiratory failure when a range of 88–92% should be achieved.
Pulse oximetry monitoring is recommended for postoperative patients despite the lack of evidence from randomised studies.
One of the commonest indications for anaesthetists to prescribe supplemental postoperative oxygen therapy is to help prevent hypoxaemia when PCA is used. In two reviews, the incidence of postoperative hypoxaemia in patients receiving PCA was found to be 11.5% and 15.2%.373 ,374
However, Cashman and Dolin's373 systematic review comparing the effects of acute postoperative pain management on respiratory function found PCA did not lead to more respiratory events when compared with intramuscular analgesia and epidural anaesthesia. They reviewed 165 studies used a variety of indicators for respiratory depression including hypoventilation, hypercarbia, oxygen desaturation and requirement for naloxone. When using respiratory rate as a measure of respiratory depression, there was no difference between all three modalities of analgesia. However, when oxygen desaturation was used as an indicator for respiratory depression the incidence of desaturation in the intravenous PCA group was significantly lower (mean 11.5% (95% CI 5.6% to 22%)) compared with epidural analgesia (mean 15.1% (95% CI 5.6% to 22%)) and intramuscular analgesia (mean 37% (95% CI 22.6% to 45.9%)). This is perhaps surprising when PCA use is the commonest indication for supplemental oxygen.
Importantly, while administering supplemental oxygen corrects hypoxaemia, it has the ability to mask respiratory depression by delaying the onset of desaturation.102 ,107 A study using transcutaneous carbon dioxide monitoring via ear lobe probe (TOSCA) compared postoperative patients using epidural analgesia and patients using morphine via PCA infusion pump.375 All patients received oxygen 4 L/min in the postoperative period. Significant desaturations were not observed in either group. However, the PCA group had a higher median PtCO2, lower respiratory rate and longer hypercarbia time as detected by the TOSCA. This study demonstrates that transcutaneous carbon dioxide monitoring is useful in detecting opioid-induced respiratory depression. It also shows that hypoventilation is common when PCA analgesia is administered. However, outside the operating theatre and intensive care where only pulse oximetry is available, the use of supplemental oxygen may mask hypoventilation. For this reason, oxygen should be administered to correct hypoxaemia rather than prevent it. A target saturation of 94–98% is recommended in most patients except those at risk of hypercapnic respiratory failure when a range of 88–92% should be achieved.
Niesters et al107 have recently demonstrated in a proof-of-concept study that hyperoxaemia has an additive effect on opioid-induced respiratory depression. In a study of 20 healthy volunteers, there was steep reduction in minute ventilation and increase in end-tidal CO2 when breathing 50% oxygen compared with breathing air while receiving a remifentanyl infusion. Additionally apnoeic episodes were significantly higher while breathing oxygen. An audit of blood gases from 4866 patients at a university hospital has shown that hypercapnia was commoner than hypoxaemia in blood gas samples from surgical wards, a surgical HDU, theatre and the ICU as well as on medical wards and many of these hypercapnic patients had respiratory acidosis.42
In the absence of large RCTs investigating the effects of PCA and the effects of hyperoxaemia, oxygen should be administered to correct hypoxaemia rather than prevent it. A target saturation of 94–98% is recommended in most patients except those at risk of hypercapnic respiratory failure when a range of 88–92% should be achieved.
Good practice points
Patients using PCA should have two-hourly oximetry observations because of the risk of hypoxaemia. Oxygen should be administered to keep patients within the appropriate target saturation range.
A target saturation of 94–98% is advised in most patients having PCA except those at risk of hypercapnic respiratory failure when a range of 88–92% should be achieved.
High levels of inspired oxygen (eg, 80%) in the perioperative and postoperative periods have in the past, been proposed to improve clinical outcomes including a reduction in the incidence of surgical site infection. The rationale for its use being that increased tissue PO2 within surgical wounds might enhance neutrophil killing capacity resulting in reduced rates of infection. Earlier meta-analysis supported this hypothesis;376 ,377 however, three RCTs have been published subsequently and do not concur with these findings.378–380
Two recent meta-analysis again show conflicting results: Togioka et al381 included seven randomised trials and found no overall benefit of hyperoxia in reducing surgical site infection. However, a statistically significant benefit was demonstrated in subgroups undergoing general anaesthesia and colorectal surgery. Hovaguimian et al382 included nine randomised trials in their meta-analysis and concluded that high perioperative oxygen did reduce the risk of perioperative surgical site infection. Both these meta-analyses included the largest RCT in this area (the PROXI trial), including 1400 patients, which showed no benefit in the administration of 80% oxygen compared with 30% oxygen in the risk of developing surgical site infection after abdominal surgery.379 Long-term follow-up of patients with cancer within the PROXI study revealed a 45% increase in long-term mortality in the high FiO2 group (HR was 1.45; 95% CI 1.10 to 1.90; p=0.009).383 Kurz et al384 reported in 2015 that supplemental oxygen did not reduce surgical site infection risk among patients having colorectal resections.
Hyperoxia has also been proposed to reduce the incidence of postoperative nausea and vomiting via a number of mechanisms including the prevention of subtle intestinal ischaemia reducing serotonin release and the reduction of dopamine release in the carotid bodies. This has been extensively investigated with conflicting evidence from RCTs. Two recent systematic reviews and meta-analyses show differing results.382 ,385 Orhan-Sungur et al385 included data from 10 studies and showed no overall benefit in hyperoxaemia reducing the risks of postoperative nausea and vomiting. Hovaguimian et al382 included data from 11 studies and showed high concentrations of oxygen provided a significant protective effect in a subgroup of patients who received inhalation anaesthetics without prophylactic antiemetics. However, overall there was no benefit in the composite end point postoperative nausea and vomiting.
Experimental data have shown hyperbaric oxygen improves anastomotic integrity in animal models.386 ,387 Recently, 72 patients who underwent elective open infraperitoneal anastomosis for rectal cancer were randomised to 30% or 80% oxygen at induction and for 6 hours postoperatively.388 The risk of anastomotic leak was 46% lower in the 80% FiO2 group (RR 0.63; 95% CI 0.42 to 0.98) versus the 30% FiO2 group. The same group has shown similar results in patients with oesophagojejunal anastomosis when the risk of anastomotic leak was 49% lower in the 80% FiO2 group (RR 0.61; 95% CI 0.40 to 0.95) versus the 30% FiO2 group.389 However, the numbers of patients in both studies in each treatment arm were small and further work is required from other investigators to validate this finding, especially in view of the concerns of Meyhoff et al383 that high-concentration oxygen may increase medium-term mortality in patients having cancer surgery.
Evidence statements
▸ The possible effects of hyperoxaemia in the perioperative and postoperative period remain controversial and may or may not reduce overall surgical site infection. However, there may be benefit in subgroups of patients undergoing general anaesthesia and colorectal surgery for non-malignant disease (evidence level 1−).
▸ Hyperoxaemia in the perioperative and postoperative period does not substantially reduce the incidence of postoperative nausea and vomiting but meta-analyses have come to conflicting conclusions (evidence level 1−).
▸ Hyperoxaemia in the perioperative and postoperative period has been shown to improve anastomotic integrity in patients undergoing gastric and colorectal surgery (evidence level 1−).
Recommendation
J1: Hyperoxaemia is not recommended routinely in the perioperative and postoperative period to reduce the incidence of postoperative nausea and vomiting (grade D).
Good practice point
There is conflicting evidence concerning the balance of potential benefits and risks of perioperative hyperoxaemia to reduce the risk of surgical site infection in elective surgery and there is no evidence for this practice in patients having emergency surgical procedures. More trials are required for specific procedures and more information is required concerning long-term mortality risks to patients with cancer. In the meantime, oxygen should not be used for this indication outside of clinical trials.
Conscious sedation may be defined as “a technique in which the use of a drug or drugs produces a state of depression of the central nervous system enabling treatment to be carried out, but during which verbal contact with the patient is maintained throughout the period of sedation. The drugs and techniques used to provide conscious sedation should carry a margin of safety wide enough to render loss of consciousness unlikely.”390 Conscious sedation is a common hospital procedure in a variety of settings from the endoscopy suite to the emergency department. It is performed by anaesthetists, physicians, trained nurses and operating department practitioners. The most commonly used sedative agents are those belonging to the benzodiazepine and opioid classes and increasingly, propofol.
During fibre-optic bronchoscopy reduction in SaO2 is a common occurrence391–393 independent of whether a transnasal or transoral approach is selected.394 There are several contributing factors including the effect of central respiratory depressant drugs, partial physical occlusion of the airway by the bronchoscope, prolonged use of airway suction, as well as V/Q mismatch produced by instillation of anaesthetic solution and lavage fluids in the airways.395–397 One small non-blinded randomised study showed no significant influence of patient positioning (supine vs semirecumbent) on the desaturation observed during fibre-optic bronchoscopy,393 although a further study has shown a higher rate of desaturation in the sitting as opposed to supine position.398
Milman et al391 demonstrated that following benzodiazepine sedation, without supplemental oxygen, 38% of patients desaturate (SpO2<90%) before bronchoscopy, 80% during and 60% following the procedure. Thus, all patients undergoing fibre-optic bronchoscopy should be routinely monitored using transcutaneous pulse oximetry which provides an accurate non-invasive method for assessing hypoxaemia during the sedation, procedure and recovery stages.
There are variable data available on the effect of hypoxaemia on the incidence of significant complications including cardiac arrhythmia during fibre-optic bronchoscopy. In an early prospective study minor rhythm abnormalities were frequently noted, with more major rhythm abnormalities more commonly seen in patients who developed hypoxaemia following the procedure.399 All arrhythmias were self-limiting and did not lead to haemodynamic compromise. This finding was reiterated in a further study which again showed a noted association between hypoxaemia and the development of cardiac arrhythmia.392 In contrast, Lundgren et al395 in a small study of 10 patients with restrictive lung disease secondary to pulmonary fibrosis demonstrated that although prolonged airway suctioning lead to a reduction in PaO2 there was no significant associated increased incidence of cardiac arrhythmia. Further studies have shown no increase in arrhythmias during fibre-optic bronchoscopy, with similar rates of minor arrhythmias to that seen during lung function testing.391 ,394
The degree and duration of hypoxaemia may be ameliorated by oxygen supplementation provided via a nasal or pharyngeal catheter.391 ,393 In a large 6-year retrospective study (n=1051) it was demonstrated that routine use of oxygen on a prophylactic basis was not required during fibre-optic bronchoscopy even when conscious sedation is performed, as most desaturations observed were transient and thus not requiring specific intervention.400 The requirement for supplemental oxygen is, however, known to increase in relation to falling FEV1 or PEF. Jones and O'Driscoll400 showed that 35% of those with an FEV1<1 L required administration of oxygen, 14% with an FEV1 of 1.0–1.5 L and 7% with an FEV1>1.5 L. However, requirement for supplemental oxygen remains variable, ranging from 5% to 32% and thus needs to be assessed on an individual basis.400 ,401
Oxygen supplementation should thus be used when desaturation is significant (SpO2<90%, change of SpO2>4%) and prolonged (>1 min) to reduce the risk of hypoxaemia-associated complications.391 ,392 ,399 ,400 ,402 The arterial oxygenation target should be dependent on the individual patient, a SpO2 of 94–98% being suitable for the majority of patients, except those at risk of hypercapnic respiratory failure where an appropriate target is a SpO2 88–92%.
Reduction in transcutaneous SaO2 has also been reported during and following both upper403–409 and lower408–410 GI endoscopy, particularly during more complicated therapeutic procedures such as endoscopic retrograde cholangiopancreatography.409 ,411 ,412 A small observational study showed more marked desaturation in those patients with a pre-existing requirement for long-term oxygen therapy.412 Hypoxaemia is likely to be multifactorial, as is the case with bronchoscopic procedures, a consequence of sedation and the physical distortion of the airway produced by passage of the endoscope. Thus, as with fibre-optic bronchoscopy it is essential to ensure adequate facilities for monitoring of transcutaneous oxygen saturations at all stages throughout the procedure.
Hypoxaemia during GI endoscopy may be more frequently observed in individuals with pre-existing cardiorespiratory disease or those undergoing complicated therapeutic procedures, especially if heavily sedated.292 ,293 ,295 ,296 ,300 ,301 Although the use of oxygen therapy on a prophylactic basis is suggested in all those patients receiving conscious sedation in the current guidelines of the British Society of Gastroenterology,301 there are, however, no recognised studies analysing whether routine use of prophylactic oxygen decreases or increases the risks of GI endoscopy even in at-risk patients. There is a risk that routine oxygen use might actually mask the development of respiratory failure in such patients because the patient could develop hypercapnia and carbon dioxide narcosis despite having satisfactory oxygen saturation measurements. Such patients require careful continuous oxygen saturation monitoring and clinical observation throughout, and facilities for oxygen administration should be readily available in the event of significant desaturation as discussed in section 7.
Limited data are available on the use of oxygen during other procedures involving conscious sedation. Invasive cardiac procedures such as cardiac catheterisation and angioplasty have been associated with arterial oxygen desaturation in a significant proportion of patients, particularly those with recognised cardiorespiratory disease, and can be corrected by supplemental oxygen administration.413 In an emergency department setting, procedures requiring conscious sedation may also be associated with hypoxaemia; however, use of oxygen in a prophylactic manner has not been demonstrated to reduce the incidence of hypoxaemic events, although these studies were small and likely to be underpowered to this end.414 ,415
SaO2 monitoring is indicated during the administration of sedation, procedure and recovery period in all procedures involving conscious sedation. Significant caution should be taken with both the administration of sedation and supplemental oxygen in patients with known resting hypercapnia or significant lung disease who are at risk of hypercapnic respiratory failure. It is crucial to ensure sufficient clinical assessment of patients at all times. Monitoring of transcutaneous carbon dioxide levels and capnography in additional to standard monitoring may be of use, particularly in high-risk patients and those receiving moderate or deep sedation to identify early signs of respiratory depression.416 ,417
Evidence statements
▸ Hypoxaemia is a common observation during fibre-optic bronchoscopy related to use of central depressant drugs, partial airway occlusion, use of airway suction, patient positioning and instillation of fluid into the airways. There is a noted relationship between reduced FEV1 and PEF and increased occurrence of hypoxaemia (evidence level 4).
▸ Hypoxaemia is also noted during both upper and lower GI endoscopy and other procedures involving conscious sedation (evidence level 2+).
▸ The use of supplemental oxygen via nasal or pharyngeal catheter can ameliorate hypoxaemia (evidence level 2+).
▸ Oxygen supplementation should be provided to patients with persistent reduction in SaO2 (SpO2<90% or change >4%, for >1 min) (evidence level 4).
Recommendations
J2: All procedures involving conscious sedation warrant routine continuous monitoring of oxygen saturation via pulse oximetry prior to and during the procedure, and in the recovery period, particularly fibre-optic bronchoscopy and upper GI endoscopy where a reduction in SaO2 is common, particularly with concurrent use of sedation (grade C).
J3: Significant arterial oxygen desaturation (SpO2<90% or fall of 4% or more that is prolonged (>1 min during endoscopy procedures)) should be corrected by supplemental oxygen with the aim of achieving target oxygen saturations of 94–98%, or 88–92% in those at risk of hypercapnic respiratory failure (grade D).
J4: Complicated upper GI endoscopy or procedures in patients with cardiorespiratory comorbidity are especially likely to lead to hypoxaemia and may also lead to hypercapnia, especially if the patient is heavily sedated. It is recommended that blood gases should be measured if such patients should require prolonged oxygen administration. The routine administration of oxygen is not recommended as it may delay the recognition of respiratory failure (grade D).
J5: Constant clinical assessment of the patient is crucial at all stages of conscious sedation procedures and monitoring of capnography or transcutaneous carbon dioxide levels may be a useful adjunct to identify early respiratory depression (grade D).
J6: During the recovery period after procedures requiring conscious sedation, supplemental oxygen should be titrated to achieve target saturations of 94–98% in most patients and 88–92% in those at risk of hypercapnic respiratory failure (see section 10.5.1) (grade D).
In 2004, a working party of the Association of Palliative Medicine Scientific Committee set out to examine the evidence concerning the use of oxygen for the palliation of breathlessness in COPD, advanced cancer and chronic heart failure.418 They found that there was evidence that oxygen may have a useful role in the palliation of breathlessness.419 ,420 However, the conclusion of most subsequent studies147 ,148 ,150 ,421 and systematic reviews159 ,422–424 is that there is no difference between oxygen or air in relief of breathlessness, although the intervention with either seems to induce some sense of relief of symptoms. There is general consensus that facial cooling (eg, by hand-held fan) of second and third branches of trigeminal/vagal nerve reduces the sensation of breathlessness.425 These mechanisms are believed to be the reasons why both air and oxygen seem to work equally.
In addition, there is also the question of the relationship of hypoxaemia to the sensation of breathlessness. There does not seem to be a clear relationship between the two as it has been shown that occurrence of hypoxaemia (or absence of hypoxaemia) has no relationship to relief of breathlessness in palliative care patients.426
Breathlessness in terminally ill patients is a complex multifaceted problem. The relief of this distressing symptom should be individualised in each patient. The evidence of benefit from opioids and non-pharmacological treatments is stronger than the evidence of benefit from oxygen, especially for non-hypoxaemic patients426 ,427 (evidence level 2+). Simple devices like hand-held fans may be tried before more complex methods (eg, oxygen and its attached equipment) are tried. There is concern in the clinical community that dying patients may become psychologically dependent on oxygen and become afraid to let go of the equipment even when clearly dying. Face masks can be intrusive and may be perceived as a barrier by the family members between them and the patient. Campbell and colleagues have shown that, when death is imminent, in the absence of respiratory distress, oxygen should not be routinely given even when severe hypoxaemia is present. Among those already receiving oxygen, it was possible to discontinue it in 90% without causing distress.428
Previous clinical recommendations for the use of oxygen in palliative care were based on the recommendations from the working party of the Association of Palliative Medicine Science Committee in 2004418 but most publications since that date have cast doubt on the value of oxygen therapy for patients with advanced cancer or heart failure unless the patient is hypoxaemic. For some conditions such as advanced pulmonary fibrosis requiring palliative care, the potential benefits of oxygen for non-hypoxaemic patients at rest have not been addressed in clinical trials although many patients with this condition desaturate on exertion and benefit from ambulatory oxygen therapy. Readers should refer to the BTS Home Oxygen guideline for guidance about the medium-term use of oxygen by palliative care patients in the home setting.13
Evidence statements
▸ Breathlessness is a common symptom among palliative care patients but there is little evidence that the degree of breathlessness is related to the oxygen saturation (evidence level 2+).
▸ Most recent studies have shown that there is no difference between oxygen and air in the relief of breathlessness in non-hypoxaemic palliative care patients (evidence level 1+).
▸ There is contradictory evidence concerning the possible benefits of oxygen in hypoxaemic palliative care patients, most studies were negative (evidence level 2+).
▸ Recent studies suggest that alternative treatments such as opioids or non-pharmacological therapy such as a hand-held fan or treatment of anxiety may be more beneficial (evidence level 2+).
Recommendations
K1: Oxygen use in palliative care patients should be restricted to patients with SpO2 consistently <90% or patients who report significant relief of breathlessness from oxygen. In non-hypoxaemic patients, opioids and non-pharmacological measures should be tried before oxygen (grade B).
K2: In general, there is no role for the monitoring of oxygen saturation or PO2 in comfort-focused care in the last few days of life. If the patient appears comfortable, oxygen levels are irrelevant and should not influence care (grade D).
Good practice points related to oxygen use in palliative care
Oxygen therapy for the symptomatic relief of breathlessness in palliative care patients is more complex than the simple correction of hypoxaemia. Consider the following issues:
Consider early involvement of palliative care specialists and physiotherapists.
As breathlessness is a multifactorial sensation, a comprehensive assessment of contributing factors (such as anxiety) should be carried out.
Low-dose opioids should be considered because they are effective for the relief of breathlessness in palliative care patients.
A trial of a hand-held fan to help relieve breathlessness is recommended prior to trial of oxygen.
Oxygen use has to be tailored to the individual and a formal assessment made of its efficacy for reducing breathlessness and improving quality of life for that person.
Oxygen therapy should not be continued in the absence of patient benefit or where its disadvantages (eg, discomfort of masks or nasal cannulae, drying of mucous membranes) outweigh any likely symptomatic benefit.
Helium is an inert gas which is lighter and less dense than oxygen and nitrogen which comprise over 99% the air that we breathe. Helium has been mixed with oxygen (Heliox), usually in a ratio of 80:20 or 70:30 to treat adults and children with upper and lower airway disease as the reduced gas density can decrease resistance to airflow and therefore the work of breathing in narrowed airways. A 4-year study in a critical care unit reported 92 instances of use (73% paediatric) with an ∼50/50 ratio of upper and lower airway disorders treated by Heliox.429
The use of Heliox for upper airway obstruction in adults has not been the subject of formal clinical trials because presentations are rare, the site and nature of airflow obstruction is variable and patients tend to present as acute emergencies where randomisation would be difficult. However, there are case reports of benefit where Heliox has been used with apparent benefit to patients (and no side effects other than temporary alteration in the voice).
Heliox has been used in asthma and COPD, both as an inhaled gas and as the driving gas for nebulised treatments. There is a great deal of uncertainty about possible benefits, partly because the gas itself can affect the calibration and functioning of equipment and this can influence measures of airflow such as peak expiratory flow and FEV1. A systematic review in 2003 concluded that the existing evidence did not provide support for the administration of helium–oxygen mixtures to emergency department patients with moderate-to-severe acute asthma with the caveat that the conclusions were based on between-group comparisons and small studies and the results should be interpreted with caution.430 A later review in 2007 and a small randomised trial published in 2011 noted a slight improvement in airflow measures but the clinical significance could not be determined.431 ,432
The use of Heliox in COPD has been less studied than its use in asthma. A retrospective study of 81 patients with AECOPD and respiratory acidosis reported a significant decrease in intubation and mortality in the Heliox group and shorter ICU stay and hospital stay in survivors.433 The authors advised (in 2001) that prospective randomised studies were needed and a later meta-analysis (in 2004) concluded that definitive evidence of benefit was lacking.434 Heliox has been used with reported benefit in conjunction with non-invasive positive pressure ventilation but that is outside the scope of this guideline.
The use of Heliox as a driving gas for nebulisers is also controversial, partly due to the complex interactions between the driving gas and the inhaled medication and measures of airflow. A systematic review in 2007 concluded that the use of Heliox to drive nebulisers in patients with acute asthma slightly improved airflow measures but it was not possible to determine whether this improved recovery.431
Evidence statements
▸ There is little evidence overall to suggest that Heliox has any benefit over air–oxygen mixtures in asthma or COPD and it is more expensive than oxygen–air mixtures (evidence level 1−).
▸ There is weak evidence from case reports and clinical practice that a therapeutic trial of Heliox may be reasonable in patients with mechanical upper airway obstruction or postoperative stridor (evidence level 3).
Recommendations
L1: There is insufficient evidence to support the use of Heliox either as an inhaled gas or as the driving gas for nebuliser therapy in adult patients with acute exacerbations of asthma or AECOPD except as part of randomised clinical trials or in exceptional circumstances (grade D).
L2: A therapeutic trial of Heliox is reasonable in patients with mechanical upper airway obstruction or postoperative stridor (grade D).
L3: Heliox use for patients with asthma or COPD should be considered only in clinical trials or in specialist hands for severe exacerbations that are not responding to standard treatment (and in patients with COPD where there are contraindications to intubation) (grade D).
The principles and indications for use of CPAP outside of urgent care are beyond the scope of this guideline as are the technical details of CPAP use. Acute CPAP therapy is used commonly in the management of acute pulmonary oedema and many patients who are overweight or long-term users of home CPAP require hospital admission for the management of medical and surgical conditions. Most of these patients should continue to use their own CPAP device during their hospital admission (usually overnight) and some may need to entrain oxygen to maintain their target oxygen saturation range. The use of CPAP in patients in the preoperative and postoperative period to treat or prevent hypoxaemia in patients with sleep-disordered breathing and the use of CPAP to treat pulmonary oedema warrant special consideration.
Obesity has reached epidemic proportions with more than one billion overweight adults worldwide, of whom at least 300 million are obese (see also section 8.15). Obesity predisposes to OSA and OHS. CPAP is the mainstay of medical treatment for patients with OSA. It has been shown to reduce apnoeas and daytime sleepiness as well as reducing sequelae of untreated OSA such as impaired cognition, hypertension, coronary artery disease and cerebrovascular accident.435 The incidence of postoperative desaturation and respiratory failure is unsurprisingly high in patients with OSA.436 Residual anaesthetic drugs have the potential to weaken the muscles of the upper airway and depress the respiratory drive, thus amplifying the disease. CPAP in the postoperative period has been shown to reduce reintubation and severe respiratory complications after major abdominal surgery in patients without sleep-disordered breathing.437 An observational study of 16 patients with OSA reported a reduction in postoperative complications in patients who used CPAP preoperatively, on extubation and continuously for 24–48 hours after surgery.438 The British Obesity and Metabolic Surgery Society (BOMSS) recommend patients with diagnosed sleep-disordered breathing established on CPAP or bi-level positive airway pressure ventilation (BiPAP) who are undergoing surgery, to bring their machines with them and use them in the preoperative and postoperative period.439 Patients with OSA or OHS with evidence of desaturation <88% in the postoperative period should be started on CPAP or BiPAP rather than supplemental oxygen alone. Supplemental oxygen can be entrained if necessary to maintain the target saturation range, usually 88–92%.
Caution should be exercised when administering oxygen to all morbidly obese patients even those without a diagnosis of sleep-disordered breathing. One study of 40 morbidly obese patients undergoing laparoscopic bariatric surgery showed the incidence of postoperative hypoxaemia was as high in patients without OSA compared with those with a diagnosis of OSA and supplemental oxygen did not reduce the frequency of oxygen desaturations.440
Evidence statements
▸ OSA is associated with increased incidence of desaturation, respiratory failure, cardiac events and ICU admission (evidence level 1+).
▸ CPAP therapy used in the preoperative and postoperative period reduces complications in patients with OSA after surgery (evidence level 2+).
Recommendation
N1: Patients with diagnosed sleep-disordered breathing established on CPAP undergoing surgery should bring their machines with them and use them in the preoperative and postoperative period. If adequate saturations are not achieved despite CPAP therapy then assess for worsening ventilation with blood gases and oxygen should be entrained to achieve a saturation of 88–92% (grade D).
Two meta-analysis studies and one large RCT (Gray et al443) have provided evidence that CPAP administered with supplemental oxygen has definite measurable physiological and short-term clinical benefits in pulmonary oedema.441 ,442 The longer term benefits are less clear, in particular any reduction in mortality. The meta-analysis and a prehospital RCT looking at use of CPAP suggest reduced mortality and/or intubation rates.441 ,442 ,444 However, this mortality benefit was not found in the largest and best constructed RCT.443 In addition, this study did not report a reduction in the number of intubations.
Evidence statements
▸ Patients with cardiogenic pulmonary oedema, treated with CPAP and O2 show early improvement in gas exchange when compared with standard treatment (evidence level 1+).
▸ Reports that short-term mortality and intubation rates are decreased were not confirmed in the largest RCT (evidence level 1+).
▸ The use of CPAP therapy in the prehospital environment may be beneficial to patients with acute pulmonary oedema as it can potentially decrease the need for endotracheal intubation, improve vital signs during transport to hospital and improve short-term mortality (evidence level 1+).
Recommendation
N2: CPAP with entrained oxygen to maintain saturation 94–98% should be considered as an adjunctive treatment to improve gas exchange in patients with cardiogenic pulmonary oedema who are not responding to standard treatment in hospital care or in prehospital care (grade B).
This section applies to a range of clinical settings to include emergency oxygen use in patients' homes, GP practices or health centres and within an ambulance care setting. Management in some prehospital settings such as a primary care centre or in a paramedic ambulance may be almost identical to hospital management. Readers are referred to section 10 for advice concerning choice of oxygen delivery devices and systems.
Readers are referred to tables 1–4 and charts 1 and 2 for a summary of the key elements of oxygen therapy in common medical emergencies. A brief summary of this section can be downloaded from www.brit-thoracic.org.uk.
Ongoing care at home of chronically hypoxaemic patients is not covered by this guideline. There is little literature on which to base any recommendations when such patients have an acute exacerbation of their condition, but patient safety should be the priority. The NICE guidelines on COPD recommend that patients receiving long-term oxygen and those with an PaO2 of <7 kPa should be considered for treatment in hospital during exacerbations.1
Good practice point
Chronically hypoxaemic patients with a clinical exacerbation associated with a 3% or greater fall in oxygen saturation on their usual oxygen therapy should usually be assessed in hospital with blood gas estimations. PaO2 of <7 kPa equates to SpO2 below ∼85%.
It is essential to provide optimal oxygen therapy at the earliest possible opportunity while the acutely breathless patient is being assessed and treated in the community and during transfer to hospital. For most such patients the main concern is to give sufficient oxygen to support their needs. Hypoxaemia can lead to cardiac arrhythmias, renal damage and, ultimately, cerebral damage. However, excessive oxygen therapy can also be dangerous for some patients, especially those with advanced COPD. Target saturation should be used; pulse oximetry is necessary to achieve this. Section 10.4.2 provides advice concerning the choice of oxygen cylinders in primary care practices.
Emergency ambulances and emergency/fast response type vehicles and ambulance service motorbikes and cycles should be equipped with oxygen and oximeters appropriate to the mode of transport. Thus, fast response cars/motorbikes and cycles will require hand-held finger oximeter-type devices and staff initiating oxygen in the home will need a portable or finger oximeter. Pulse oximetry devices used by Community First Responder (CFR) schemes should wherever possible reflect that of the ambulance service to which they are affiliated. Likewise Voluntary Aid Societies (VAS) medical directors are encouraged to discuss the purchase and use of pulse oximeters.
There are many cheap, small, finger oximeters available on the internet, but there has been no thorough evaluation of the accuracy and reliability of these devices. However, they are now being widely used by medical staff in many settings, and by patients on oxygen therapy at home. In the future, having a small oximeter may be as ubiquitous as a stethoscope, reinforcing that oxygen saturations should be the ‘fifth vital sign’. Within hospital medicine, the oximeter reading is now established as an essential part of the NEWS.96
Evidence statement
The use of oximeters in acute care is based on physiological data and expert opinion in the absence of randomised trials (evidence level 4).
Recommendations
T1: Pulse oximetry must be available in all locations where emergency oxygen is being used by healthcare professionals (see also the limitations of using pulse oximetry section 7.1.2) (grade D).
V1: Emergency oxygen should be available in primary care medical centres, preferably using oxygen cylinders with integral high-flow regulators. Alternatively, oxygen cylinders fitted with high-flow regulators (delivering up to 15 L/min) must be used to allow use with reservoir masks (grade D).
V2: Healthcare organisations should take measures to eliminate the risk of oxygen tubing being connected to the incorrect wall oxygen outlet or to outlets that deliver compressed air or other gases instead of oxygen. Air flow meters should be removed from the wall sockets or covered with a designated air outlet cover when not in use. Special care should be taken if twin oxygen outlets are in use (grade D).
It is suggested that the first healthcare professional(s) to encounter an acutely breathless patient should perform an initial ‘ABC’ assessment, followed by obtaining a quick history from the patient and/or family or friends. Immediate assessment should include recording of pulse rate, respiratory rate and pulse oximetry.
Clinical assessment of a breathless patient starts with ‘ABC’ (see recommendation B1).
A brief history should be taken from the patient or other informant.
Initial assessment should include pulse and respiratory rate in all cases (see recommendation B1).
Pulse oximetry should always be measured in patients with breathlessness or suspected hypoxaemia (see recommendation B2).
Disease-specific measurements should also be recorded (eg, peak expiratory flow in asthma, blood pressure in cardiac disease).
Having ascertained that the airway is clear, the first responders should start oxygen treatment if the oxygen saturation is below the target. The initial oxygen therapy should follow the general principles given in tables 1–4 and charts 1 and 2. There is some evidence that bronchodilator therapy, however given, can cause increased V/Q mismatch and reduced blood oxygen levels in acutely ill patients shortly after treatment (see section 10.8.1).
Good practice points
The initial oxygen therapy to be used in the various clinical situations is given in tables 1–4.
If there is a clear history of asthma or heart failure or other treatable illness, appropriate treatment should be instituted in accordance with guidelines or standard management plans for each disease.
The oxygen saturation should be monitored continuously until the patient is stable or arrives at hospital for a full assessment. The oxygen concentration should be adjusted upwards or downwards to maintain the target saturation range.
In most emergency situations, oxygen is given to patients immediately without a formal prescription or drug order. The lack of a prescription should never preclude oxygen being given when needed in an emergency situation. However, a subsequent written record must be made of what oxygen therapy has been given to every patient (in a similar manner to the recording of all other emergency treatment).
A proportion of breathless patients will have COPD. A 2006 Cochrane review of oxygen therapy for COPD in the prehospital setting found no relevant randomised studies but the paper by Austin et al51 in 2010 has shown a reduced mortality in patients with COPD in prehospital care who were managed with titrated oxygen to achieve a target saturation of 88–92% compared with high-concentration oxygen therapy (RR 0.22).445
Audits of emergency admissions in UK hospitals have shown that at least 5% of all medical admissions and 25% of breathless or hypoxaemic medical patients who require hospital admission have COPD or other conditions that may place them at risk of hypercapnia.165 UK government data list over 100 000 hospital admissions due to COPD each year which constitutes 2% of all emergency admissions to hospitals in England and Wales.446 Many of these patients will require carefully titrated oxygen therapy because they are at risk of carbon dioxide retention or respiratory acidosis. In a large UK study, 47% of patients with exacerbated COPD had PaCO2>6.0 kPa (45 mm Hg), 20% had respiratory acidosis (pH<7.35 or [H+]>45 nmol/L) and 4.6% had severe acidosis (pH<7.25 or [H+]>56 nmol/L).43 Acidosis was more common if the blood oxygen was >10 kPa (75 mm Hg). Plant et al43 recommended that patients with acute COPD should be maintained within a PaO2 range of 7.3–10 kPa (55–75 mm Hg) to avoid the dangers of hypoxaemia and acidosis.
Good practice points (section 8.12 and table 3)
Patients with COPD should initially be given oxygen via a Venturi 24% mask at 2–3 L/min or Venturi 28% mask at a flow rate of 4–6 L/min or nasal cannulae at a flow rate of 1–2 L/min.
Some patients may benefit from higher flow rates via the Venturi mask (see section 10.2.3). The target oxygen saturation should be 88–92% in most cases or an individualised saturation range based on the patient's blood gas measurements during previous exacerbations.
One of the challenges faced by the initial clinical response staff is that the diagnosis may be unclear and the patient's medical records or detailed history may not be available. It has been shown that ambulance teams may be aware of a diagnosis of COPD in only 58% of cases.447
The Guideline Group consider that an initial diagnosis of COPD should be assumed if there is no clear history of asthma and the patient is >50 years of age and a long-term smoker or ex-smoker with a history of longstanding breathlessness on minor exertion. The diagnosis should be reassessed on arrival at hospital where more information will probably become available, and the FEV1 should be measured unless the patient is too breathless to undertake spirometry.
Good practice point
If the diagnosis is unknown, patients >50 years of age, who are long-term smokers with a history of chronic breathlessness on minor exertion such as walking on level ground, and no other known cause of breathlessness, should be treated as having suspected COPD for the purposes of this guideline. Patients with COPD may also use terms such as chronic bronchitis and emphysema to describe their condition but may sometimes mistakenly use ‘asthma’ (see table 3).
Patients who are already on long-term oxygen therapy most of whom will have COPD.
Patients with fixed airflow obstruction associated with bronchiectasis.
Any patient with severe kyphoscoliosis or severe ankylosing spondylitis.
Severe lung scarring from old tuberculosis (especially with thoracoplasty).
Morbid obesity (BMI>40 kg/m2).
Patients with neuromuscular disorders (especially if muscle weakness has led to wheelchair use).
Any patient on home mechanical ventilation.
Overdose of opioids, benzodiazepines or other drugs causing respiratory depression.
The administration of high oxygen concentrations in acute COPD and other conditions (see section 8.12) leads to worsening of hypercapnic respiratory failure and respiratory acidosis.43 Patients with COPD on oxygen therapy with a PO2>10 kPa (75 mm Hg) are at risk of CO2 retention may be assumed to have excessive oxygen therapy. This is a very common problem, data from the 2008 national COPD audit indicate that 30% of patients with COPD had received >35% oxygen in the ambulance prior to admission and 35% were still receiving high-concentration oxygen when blood gases were taken in hospital.46
If a patient is found to have respiratory acidosis due to excessive oxygen therapy, the oxygen therapy should not be discontinued immediately because the oxygen level will fall significantly over 1–2 min by virtue of the alveolar gas equation (see section 5.2.1), whereas the carbon dioxide level will take much longer to correct itself (see section 5.3.2). In this situation, the oxygen treatment should be stepped down to 28% or 35% oxygen from a Venturi mask, or oxygen at 1–2 L/min from nasal cannulae depending on oxygen saturation and blood gas results. A saturation target of 88–92% is recommended for acidotic patients in hypercapnic respiratory failure and NIV is required if the acidosis does not resolve quickly.1 ,43 This avoidable problem has occurred historically during the transfer to hospital, prior to measurement of ABGs or before a definitive diagnosis is known. Furthermore, ambulance staff are often not informed at present of a diagnosis of COPD and may not be aware of the presence of other high-risk conditions such as kyphoscoliosis or respiratory failure due to neuromuscular conditions.447 These patients should be issued with an oxygen alert card (example shown in figure 8) and a 24% or 28% Venturi mask based on previous blood gas results. The recommended oxygen saturation will be based on the clinical scenario for each individual patient but will usually be 88–92%, occasionally 85–88% or 85–90% based on previous blood gas results. Patients should be instructed to show this card to the ambulance crew and emergency department staff in order to avoid the use of high oxygen concentrations. This scheme can be successful.448 The ambulance service should be informed about which patients are issued with oxygen alert cards. The Association of Ambulance Chief Executives (AACE) JRCALC UK Ambulance Services Clinical Practice Guidelines 2016: (London, AACE, 2016) reflect this 2017 BTS Guideline for the use of oxygen in COPD.12
Good practice points (see also section 8.12)
Patients with COPD (and other at-risk conditions) who have had an episode of hypercapnic respiratory failure should be issued with an oxygen alert card and with a 24% or 28% Venturi mask. They should be instructed to show the card to the ambulance crew and emergency department staff in the event of an exacerbation.
The content of the alert card should be specified by the physician in charge of the patient's care, based on previous blood gas results.
If a patient has an oxygen alert card, initial oxygen therapy should be based on the guidance on the card until the results of blood gases are available.
Oxygen alert cards with agreed content can be obtained via the BTS website.
The primary care team and ambulance service should also be informed by the responsible clinician that the patient has had an episode of hypercapnic respiratory failure and carries an oxygen alert card. The home address and ideal oxygen concentration or target saturation ranges of these patients can be flagged in the ambulance control systems and information disseminated to ambulance crews when required.
Out-of-hours services providing emergency primary care services should be informed by a responsible clinician that the patient has had an episode of hypercapnic respiratory failure and carries an oxygen alert card. Use of oxygen in these patients will be guided by the instructions on the alert card or by a patient-specific protocol which can be shared by hospital teams, the ambulance service and the primary care team.
During treatment by ambulance staff, oxygen-driven nebulisers should be used for patients with asthma and may be used for patients with COPD in the absence of an air-driven compressor system. If oxygen is used for patients with known COPD, its use should be limited to 6 min. This will deliver most of the nebulised drug dose but limit the risk of hypercapnic respiratory failure (section 10.8.2). Ambulance services are encouraged to explore the feasibility of introducing battery-powered, air-driven nebulisers or portable ultrasonic nebulisers.
If a patient is suspected to have hypercapnia or respiratory acidosis due to excessive oxygen therapy, the oxygen therapy should not be discontinued but should be stepped down to the lowest level required to maintain a saturation range of 88–92%. This may be achieved using 28% or 24% oxygen from a Venturi mask or 1–2 L/min via nasal cannulae depending on oxygen saturation and subsequent blood gas results.
The range of oxygen delivery devices is very wide as discussed in section 10. However, most patients can be managed with one of five types of oxygen delivery device.
Good practice points
It is recommended that the following delivery devices should be available in prehospital settings where oxygen is administered (see section 10):
High-concentration reservoir mask (non-rebreathe mask) for high-concentration oxygen therapy;
Nasal cannulae (preferably) or a simple face mask for medium-concentration oxygen therapy;
Twenty-eight per cent Venturi mask for patients with definite or likely COPD (patients who have an oxygen alert card may have their own 24% or 28% Venturi mask);
Tracheostomy masks for patients with tracheostomy or previous laryngectomy.
The emergency use of oxygen in the patient's home will be determined by what is available in the patient's home (see section 10.4) or what is carried by the first responder. GPs are probably unlikely to carry an emergency oxygen supply such as a portable cylinder unless they work in remote or rural areas. If oxygen is available in the patient's home by either oxygen concentrator or short burst oxygen by cylinder, the flow rate should be guided by the use of pulse oximetry if available. Otherwise, the need for oxygen may need to be determined by the presence of central cyanosis which can be very difficult in poor light. Enough oxygen should be given to achieve 88−92% if the patient is known to be at risk of hypercapnia, or the target saturation as stated on their oxygen alert card. Otherwise flow rate should be titrated to achieve saturations of 94–98% or correction of cyanosis if no pulse oximeter is available. It is not recommended that patients adjust their own flow rate of an existing oxygen supply based on saturations or increase in breathlessness unless it is part of an agreed escalation plan.
Good practice points
GPs or first responders visiting a patient's home should carry a portable pulse oximeter to assess hypoxaemia and guide use of oxygen if available and should call emergency services if hypoxaemia or other serious illness is suspected.
Those attending patients as an emergency in rural or remote areas should consider carrying a portable oxygen cylinder as part of their emergency equipment.
The BTS Guideline was written for use by healthcare professionals, mostly operating within the NHS and emphasises the strategy of titrating supplemental oxygen to target levels of oxygen saturation, facilitated by the use of pulse oximeters.2 However, it is recognised that emergency oxygen is used in many other circumstances, especially by volunteers involved in Mountain Rescue, Lifeboat Rescue, Cave Rescue and similar services. In these circumstances, training of volunteers is the responsibility of the individual organisation and it is recognised that oximeters may not be available in all circumstances where oxygen is used by such teams. Furthermore, there are many circumstances such as hypothermia and shock where oximetry readings may be unreliable and these circumstances are more likely to be present during call-outs by the above services than during general ambulance operations in the UK. The AACE JRCALC UK Ambulance Services Clinical Practice Guidelines 2016: London, AACE, 2016 contains succinct guidance for ambulance staff in the UK based on the BTS Guideline.12 It is recommended that other first responder organisations may wish to base their oxygen strategies on the principles of the BTS guideline and the succinct practical advice, tables and flowchart contained in the JRCALC drugs section, accepting the limitations previously listed and the challenging environment in which these teams may operate. It is appreciated that oxygen may be used on a more pragmatic basis if it is not possible to obtain a reliable oximetry reading due to conditions such as shock or hypothermia or if oximetry is not available. Organisations are advised to prepare guidance for situations when oximetry is unreliable or unavailable for the above reasons. Organisational guidance should reflect the general principles of the BTS and JRCALC guidelines but BTS cannot endorse the specific recommendations of other bodies, especially if oxygen is given without monitoring by pulse oximetry. It is recognised that voluntary organisations may have difficulty in providing training (and regular refresher training) in the use of oxygen and oximeters to large numbers of volunteers. However, BTS regards the use of oximetry to guide oxygen therapy as best practice. Organisations should give very careful consideration to any decision resulting in a pulse oximetry not being used at the casualty site and/or in transport of seriously ill patients based on purely financial reasons.
Entonox is a 50:50 mixture of oxygen and nitrous oxide that has been widely used as an inhalational analgesic agent for many years. However, a Danish review in 1994 reported as follows: “There are no controlled studies concerning the effect of pain treatment in the pre-hospital phase. The few available controlled studies conducted inside the hospital have not shown significant pain-relieving effects of nitrous oxide for patients suffering from pain of acute medical or surgical origin when compared to other methods of pain treatment.”449 Su et al450 reported better pain control and a lower caesarean section rate when 50% nitrous oxide was given to 658 women in labour compared with 642 women given 50% oxygen. The commonest side effect was dizziness which affected 39% of those given nitrous oxide and none of the control participants. Because of its rapid onset of action and lack of serious side effects, it has been widely used in providing analgesia during childbirth and in trauma patients, in the emergency department and in the ambulance or scene of an accident. The gas mixture is usually self-administered using a facemask with a demand valve that the patient holds to their face. The demand valve opens to allow gas to flow when it detects an inspiration. The analgesic onset is rapid, occurring within a few breaths. The main side effect is drowsiness and if the patient takes too much, because they are holding the mask to their face, the mask will slip off and the patient returns to breathing ambient air again. The rapid washout of nitrous oxide means that the patient regains consciousness very quickly. The mixture is less dense than air and may expand in air filled cavities, and as such, is contraindicated in patients with known emphysema.451
There is a concern of course that if Entonox is used in patients who are at risk of hypercapnic respiratory failure, the high concentration of oxygen may precipitate hypercapnia. Again, if the patient does become drowsy because of hypercapnia or the sedating effect of Entonox, they may release the mask and return to breathing air again. Unfortunately, if the patient has a cause for hypoxaemia, this will result in swinging from hyperoxaemia to hypoxaemia. Thus for this reason, the guideline group advise that Entonox is best avoided in patients who are at risk of hypercapnia or hypoxaemia.
Evidence statement
The use of Entonox gas mixture is based on expert opinion in the absence of randomised trials to study the effects on oxygen physiology. The value of Entonox as an analgesic agent is outside the scope of this guideline (evidence level 4).
Recommendation
M1: The use of Entonox gas mixture for analgesia should be avoided if possible in patients at risk of hypercapnic respiratory failure (grade D).
The use of oxygen in the management of pregnant women in prehospital care should follow the same principles as in hospital care (section 8.14). All healthcare professionals caring for women in pregnancy should be aware of the importance of left lateral tilt or manual displacement of the uterus in circumstances of trauma, collapse, etc. This applies at gestations above 20 weeks (ie, when the fundus of the uterus reaches the level of the umbilicus). This will potentially improve maternal cardiac output and improve the mechanics of breathing. Pregnant women suffering major trauma or severe hypoxaemia should be started on high-concentration oxygen via a non-rebreathing reservoir mask and those with milder hypoxaemia can use nasal cannulae or a simple face mask or Venturi mask to achieve an oxygen saturation of 94–98% in most cases.
If mild/moderate analgesia is required during transportation, ‘Entonox’ may be administered—see previous section 9.11.
Recommendations for oxygen use in pregnancy are given in section 8.14.
Oxygen delivery systems can be considered as two components: the method of storage and provision of oxygen (eg, cylinders); the method of delivery to the patient (eg, Venturi mask). The options available for both will depend on the environment in which it is being used and the needs of the patient.
Cylinders contain compressed gas held under a very high pressure. They come in an array of sizes and hence capacity, ranging from small portable cylinders for individual patient use to large cylinders suitable for hospital use (table 12). These can be used for bedside administration where piped oxygen is not available or can be the supply for a piped system.
Examples of oxygen cylinder sizes and capacities
With recent changes in technology, high-pressure cylinders are now available (ie, filled to 200 bar rather than 137 bar which can contain 54% more gas for the same size cylinder). It is important for all users of oxygen to be aware that most oxygen cylinders are colour-coded (black cylinder with white shoulder) but some high-pressure oxygen cylinders are all white. Small lightweight cylinders are also available for ambulatory use (eg, some weigh 3.2 kg when full). All systems containing compressed gases in the UK are subject to the Pressure Systems Safety Regulations 2000 (SI 2000 No 128). These regulations are intended to prevent the risk of injury from pressurised systems. Oxygen supports combustion and there is a risk of fire if oxygen is used close to combustible materials and a source of ignition. There is one case report of a serious fire caused by spontaneous sparking in the outflow system of an oxygen cylinder.452 Although oxygen is not an explosive gas, it is possible for oxygen cylinders to explode if heated during a fire, and deaths have been recorded in these circumstances.453 ,454
Healthcare organisations must ensure that they have a policy in place which ensures the safety of patients, staff and contractors in the provision, storage, use and maintenance of compressed gas systems as required by the Health and Safety at Work Act 1974.
Clinicians using oxygen cylinders should check the labelling of the cylinder to ensure that it is an oxygen cylinder and checks should be made to ensure that the cylinder is not empty or near empty.
Liquid oxygen is contained in pressure tanks and is obtained from atmospheric oxygen by fractional distillation. It has to be evaporated into a gas before use. Large tanks are often used by hospitals and small tanks can be used domestically. Portable liquid oxygen is also available in small portable containers which can be filled from the larger tanks.
Oxygen concentrators are largely used in the domiciliary setting for the provision of long-term oxygen therapy and are therefore not used in the acute setting so will not be covered further.
This type of mask delivers oxygen at concentrations between 60% and 90% when used at a flow rate of 15 L/min (figure 9).455 The delivered oxygen concentration is variable and will depend on the mask fit and the patient's breathing pattern. These masks are most suitable for trauma and emergency use in patients in whom carbon dioxide retention is unlikely.
High-concentration reservoir mask (non-rebreathing mask).
This type of mask delivers oxygen concentrations between 40% and 60% (figure 10). It is sometimes referred to as an MC Mask, Medium Concentration Mask, Mary Catterall Mask or as a ‘Hudson Mask’, but the latter description is discouraged because the Hudson Company make many types of mask (including high-concentration reservoir masks). The guideline group favours the term ‘simple face mask’. The oxygen supplied to the patient will be of variable concentration depending on the flow of oxygen and the patient's breathing pattern. The concentration can be changed by increasing or decreasing the oxygen flows between 5 and 10 L/min. However, different brands of simple face mask can deliver a different oxygen concentration at a given flow rate. Flows of <5 L/min can cause increased resistance to breathing, and there is a possibility of a build-up of carbon dioxide within the mask and rebreathing may occur.115
Simple face mask.
This mask is suitable for patients with respiratory failure without hypercapnia (type 1 respiratory failure) but is not suitable for patients with hypercapnic (type 2) respiratory failure. The mask may deliver a high concentration of oxygen (>50%) and is therefore not recommended for patients who require low-concentration oxygen therapy because of the risk of carbon dioxide retention. Patients using a simple face mask may have an inspiratory flow rate greater than the gas flow rate from the mask, so the simple face mask should not be used at flow rates below 5 L/min.115 Several publications have shown that patients who require medium-concentration oxygen therapy tend to prefer nasal cannulae to simple face masks and the cannulae are more likely to be left in position by the patient and less likely to fall off.456–459
A Venturi mask will give an accurate concentration of oxygen to the patient regardless of oxygen flow rate (the minimum suggested flow rate is written on each Venturi device and the available options are shown in table 13; figure 11A,B). The oxygen concentration remains constant because of the Venturi principle. The gas flow into the mask is diluted with air which is entrained via the cage on the Venturi adaptor. The amount of air sucked into the cage is related to the flow of oxygen into the Venturi system. The higher the flow the more air is sucked in. The proportions remain the same and therefore the Venturi mask delivers the same concentration of oxygen as the flow rate is increased.
Total gas flow rate from Venturi masks at different oxygen flow rates
Venturi masks are available in the following concentrations: 24%, 28%, 31%, 35%, 40% and 60%. They are suitable for all patients needing a known concentration of oxygen, but 24% and 28% Venturi masks are particularly suited to those at risk of carbon dioxide retention. A further benefit of Venturi masks is that the flow rate of gas from the mask will usually exceed the inspiratory flow rate of the patient. One study has shown that patients with a respiratory rate >30 breaths/min often have an inspiratory flow rate above the minimum flow rate specified on the mask packaging.303 Therefore, for patients with a high respiratory rate, it is suggested that the flow rate for Venturi masks should be set above the minimum flow rate listed on the packaging (increasing the oxygen flow rate into a Venturi mask does not increase the concentration of oxygen which is delivered). The accuracy of oxygen delivery from a Venturi mask is greatly reduced if the mask is not accurately placed on the patient's face.460
Patients with a respiratory rate >30 breaths/min often have a flow rate which is above the minimum delivered by the Venturi system as specified by the flow rate recommended for the mask. The flow may be increased as shown in figure 11B.
Venturi masks deliver a constant percentage of oxygen but the effect on the patient will depend on the condition being treated and on the breathing pattern and baseline oxygen saturation of the patient. As might be expected from the oxygen dissociation curve, patients with an oxygen saturation that is already in the normal range will have a very small rise in oxygen saturation (although the PaO2 is likely to rise substantially). However, patients with very low oxygen saturation will have a marked rise if given even a small concentration of oxygen. This is because the oxygen dissociation curve is actually a ‘rapid escalator’ rather than a ‘slippery slope’.102 ,106 This is illustrated in figure 12 which demonstrates that a small increase in inspired oxygen concentration can make a big difference when the saturation is below 80% but the response to oxygen is much less if the saturation is close to or above 90%.
Nasal cannulae can be used to deliver low-concentration and medium-concentration oxygen concentrations (figure 13). However, there is wide variation in patients' breathing patterns so the same flow rate of nasal oxygen may have widely different effects on the blood oxygen and carbon dioxide levels of different patients. Nasal cannulae at 1–4 L/min can have effects on oxygen saturation approximately equivalent to those seen with 24–40% oxygen from Venturi masks.230 ,463 The actual concentration of oxygen delivered (FiO2) cannot be predicted and so cannot be used if a calculation of A–a gradient is required. The oxygen concentration continues to rise up to flows above 6 L/min. Some patients may experience discomfort and nasal dryness at flows above 4 L/min, but they can be well tolerated (see section 10.2.5).230 ,464 Although one might expect mouth breathing to reduce the efficiency of nasal cannulae, the majority of studies have shown that mouth breathing results in either the same inspired oxygen concentration or a higher concentration, especially when the respiratory rate is increased.464 This is important because patients with acute breathlessness are likely to breathe quickly and via the mouth rather than the nose. As there is marked individual variation in breathing pattern, the flow rate must be adjusted based on oximetry measurements and, where necessary, blood gas measurements. A cross-over comparison of nasal cannulae versus a Venturi mask (both adjusted to give satisfactory initial oxygen saturation) showed that the oxygen saturation of patients with exacerbated COPD fell below 90% for 5.4 hours/day during treatment with nasal cannulae compared with 3.7 hours/day during treatment with a Venturi mask.465 However, that study was published in 1999 before oximetery was widely used to monitor oxygen saturation.
Nasal cannulae.
The upper range of oxygen delivery from nasal cannulae is a little lower than the output of a simple face mask, but the lower range goes a lot lower than a simple face mask which should not be used below a flow rate of 5 L/min (about 40% oxygen).115 The performance and variation of nasal cannulae for medium-concentration oxygen therapy is broadly similar to that of the simple face mask, both in laboratory experiments230 ,464 and in clinical practice.457–459 ,466 ,467 One study suggested that the saturation was lower with nasal cannulae than with simple face masks in a subgroup of men following abdominal surgery.467 However, the use of target ranges would resolve this issue. Three patient preference studies comparing nasal cannulae with simple face masks in postoperative care found that patient preference was strongly in favour of nasal cannulae with up to 88% of patients preferring cannulae to masks.457–459 Another advantage of cannulae over simple face masks is that they are less likely to be removed accidentally and they allow the patient to speak and eat.458 ,468 There are no comparisons of these devices in acute care, but there is no reason to believe that the results would be any different for patients requiring medium-concentration oxygen therapy. Nasal cannula (not Venturi masks) were used in the Austin et al's51 study which showed improved survival from controlled oxygen therapy in AECOPD.
Advantages of nasal cannulae compared with simple face masks for medium-concentration oxygen therapy
Comfort (but a minority of patients dislike the flow of oxygen into the nose, especially above 4 L/min).
Adjustable flow gives wide oxygen concentration range (flow rate of 1–6 L/min gives FiO2 from ∼24% to ∼50%), suitable for variable oxygen therapy and concentration titration.
Patient preference.
No claustrophobic sensation.
Not taken off to eat or speak and less likely to fall off.
Less affected by movement of face.
Less inspiratory resistance than simple face masks.
No risk of rebreathing of carbon dioxide.
Cheaper.
Disadvantages of nasal cannulae
May cause nasal irritation or soreness.
May not work if nose is severely congested or blocked.
Actual concentration of oxygen (FiO2) cannot be predicted
There is increasing use of HFNC as an alternative delivery device for adults requiring medium-concentration and high-concentration oxygen therapy (figure 14). There is currently a small body of evidence to support its use as well as growing interest from positive clinical observations. The therapeutic effects are thought to be multifactorial and include delivery of increased FiO2, a CPAP effect and greater comfort for the patient when compared with face masks. To deliver HFNC, three elements are required: a patient interface, a gas delivery device and a humidifier. However, specific research on the effect of humidification and high-flow oxygen therapy is lacking (see section 10.6.1). A flow of at least 60 L/min can be accommodated via standard dimension prongs on adult nasal cannula. Several manufacturers provide these, specifically designed for high-flow application. Ritchie et al469 reported a positive airway pressure of about 7 cm H2O in normal volunteers at a flow of 50 L/min. Trials to date are few and small; however, Tiruvoipati et al470 performed a prospective randomised trial of 50 patients postextubation, who required high-flow oxygen therapy. This study showed HFNC to be as effective as high-flow face mask in delivering oxygen to extubated patients as well as a significant difference in tolerance of HFNC and a trend towards improved comfort in this group. A recent study by Hernández et al471 randomised 527 mechanically ventilated patients at low risk of reintubation to either high-flow nasal oxygen or conventional oxygen for 24 hours after extubation.
High-flow humidified nasal cannulae, flow generator and humidifier system.
They reported that the use of HFNC oxygen compared with conventional oxygen therapy reduced the risk of reintubation within 72 hours (4.9% vs 12.2%; p=0.04). A prospective sequential comparison trial by Roca et al472 examined 20 patients with acute hypoxaemic respiratory failure and compared HFNC with conventional oxygen therapy. HFNC was better tolerated and more comfortable than face mask. HFNC was associated with better oxygenation and lower respiratory rate. Cuquemelle et al473 also reported greater patient comfort using this system. In further support a study by Parke et al,474 60 patients with mild-to-moderate hypoxemic respiratory failure were randomised to receive HFNC or high-flow face mask and they analysed the success of allocated therapy, NIV rate and oxygenation. Significantly, more HFNC patients succeeded with their allocated therapy and the rate of NIV in this group was 10%, compared with 30% in the high-flow face mask group. The HFNC patients also had significantly fewer desaturations.
Frat et al475 randomised 310 patients with acute hypoxaemic respiratory failure (without hypercapnia) to treatment with HFNC, reservoir mask or NIV and they found that HFNC increased the number of ventilator-free days and reduced 90-day mortality but did not significantly reduce the intubation rate which was the primary end point of the study.
Larger and more comprehensive studies are still awaited but research to date is encouraging, indicating that HFNC may have an important role to play in the delivery of high-flow oxygen both in terms of physiological advantages and the tolerance and comfort of the individual patients who are not at risk of hypercapnia (evidence level 2− to 1−).
Good practice point
High-flow nasal oxygen should be considered as an alternative to reservoir mask treatment in patients with acute respiratory failure without hypercapnia.
These devices are designed to allow oxygen to be given via a tracheostomy tube or to patients with previous laryngectomy (ie, neck breathing patients; figure 15). The oxygen flow rate should be adjusted to achieve saturation in accordance with tables 1–4 and chart 1 (figure 1). Oxygen given in this way for prolonged periods needs constant humidification and patients may need suction to remove mucus from the airway.
Tracheostomy mask.
Transport of oxygen cylinders in vehicles comes under the Transport of Dangerous Substances Act or the Carriage Regulations only if 1000 L or more (measured by the water capacity of the cylinder) is carried at any one time. Ambulances are therefore exempt from this. Normal health and safety requirements will still apply.476 ,477
All cylinders must be secured appropriately so they cannot move in transit (includes portable cylinders).
No smoking in the vicinity of cylinders.
Cylinders must be checked regularly for obvious signs of leakage.
Cylinders must be kept out of direct sunlight.
Green warning triangle ‘compressed gas’ should be displayed on the vehicle.
Cylinders should never be lifted by the neck.
They should only be changed by suitably trained personnel.
Apart from portable cylinders, all cylinders should be moved using a cylinder trolley.
Cylinders must be turned off/fully closed when not in use
Cylinders must be in date. Staff should check the expiry date prior to use.
Currently, within the UK, the ambulance service—whether NHS or private—has a range of vehicles and oxygen delivery systems at their disposal. There is an increasing use of cycle response units which tend to use the lightweight AZ or C sized cylinder with a capacity of 170 L. Motorcycle response units are generally equipped with the same AZ or C sized cylinders. Fast response units based on cars tend to be equipped with at least two of the lightweight CD sized cylinders which hold 460 L. The CD cylinder is also the size favoured by mountain, cave and mines rescue teams.
Front-line ambulances are usually equipped with piped oxygen fittings (Schraeder type) and supplied from two HX sized (2300 L) cylinders, as well as carrying at least two CD sized cylinders to power a portable oxygen-powered resuscitator. The piped supply has several outlet points placed in strategic positions to which are attached standard Schrader flow meters (0–15 L/min). This enables oxygen to be given throughout the patient's journey. The ambulance is also equipped with a portable supply which can be used at the site of an accident, taken into a patient's home or can be used when transferring a patient. They carry a range of patient interfaces for delivering the oxygen under the different circumstances encountered.
Portable resuscitators are always capable of supplying free-flow oxygen therapy as well as their resuscitator facility. Again, there are a variety of portable oxygen-powered resuscitators and it is beyond the scope of these guidelines to describe each one available for use in prehospital care. It is strongly suggested that those practitioners who need to work closely with the ambulance service should become familiar with the equipment used by their local ambulance service provider. With the possible exception of the cycle response units, all types of ambulance service response will have portable resuscitators, bag-valve mask devices and hand-operated suction as a minimum. Front-line emergency ambulances will also have rechargeable battery-powered suction available.
Patient transport service ambulances are equipped with an oxygen supply, normally an HX cylinder (2300 L) delivering the oxygen via a flow meter attached directly to the cylinder. Such vehicles also tend to carry basic hand-held suction devices. A range of oxygen masks are usually available for the different types of patients carried on such vehicles. Vehicles that are equipped with an oxygen supply should also carry oximeters to ensure appropriate use of oxygen (see section 9.8 for advice on which oxygen delivery devices should be carried in ambulances).
When travelling by car, patients have the freedom to carry their own portable oxygen cylinder.476 ,477 Some GPs in rural areas also carry oxygen in their cars. However, it is advised that certain safety precautions should be followed:
Patients are allowed to carry oxygen cylinders for their own use without putting any labels or signs on their vehicle. This includes public transport such as buses or taxis. It is an offence to display a hazard diamond if oxygen is not being transported in a vehicle so it is preferable not to use a hazard triangle on private vehicles.
The cylinder should be secure within the car and cannot move during transport or in the event of an accident. The authors of this guideline are aware of one fatality caused by a patient smoking in a vehicle where an unsecured liquid oxygen cylinder spilt into the floor-well during sudden braking.
Patients should inform their car insurance company if oxygen is carried in the car.
The majority of medical centres and practices should have a supply of oxygen for emergency use. Generally, cylinders with integral high-flow regulators should be ordered. Otherwise, the cylinder must be fitted with a high-flow regulator capable of delivering a flow of up to 15 L/min in order to deliver medium-concentration and high-concentration oxygen therapy. A recommended list of oxygen delivery devices for use in prehospital care is given in section 9.8.
Emergency oxygen should be available in primary care medical centres, preferably using oxygen cylinders with integral high-flow regulators. Alternatively, oxygen cylinders fitted with high-flow regulators (delivering up to 15 L/min) must be used to allow use with reservoir masks (see recommendation V1).
In patients' homes, oxygen is usually provided for long-term therapy with an oxygen concentrator and an ambulatory supply with lightweight cylinders (or a portable liquid oxygen system). Long-term oxygen therapy is covered in other guidelines. In some circumstances, there may be a supply of cylinders for short-term/short-burst therapy or palliative use. The existing home oxygen supply may be used by a patient or GP in an emergency situation before the arrival of an ambulance using the patient's existing interface. If a GP is attending a patient at home with oxygen, ideally, the use of oxygen should be guided by pulse oximetry. The existence of any oxygen alert card should be asked for so that the emergency services attending can be aware of the target saturation and oxygen supply titrated accordingly.
The patient/carers should be made aware of the following Health and Safety recommendations:476 ,477
All cylinders should be stored on a cylinder trolley or suitably secured so they cannot be knocked over.
There should be no trailing oxygen tubing.
A green warning triangle for ‘compressed gas’ should be displayed by the front door (warns emergency services in the event of a fire).
The minimum number of cylinders should be stored in the house.
There should be no smoking in the vicinity of oxygen cylinders.
Cylinders must be checked regularly for obvious signs of leakage.
Cylinders must be kept out of direct sunlight.
Oxygen must not be used near a naked flame or source of heat.
Most hospitals have piped oxygen systems as described previously, although some wards can still be found where piped oxygen is not available and large compressed gas cylinders are used to supply the oxygen. Acute hospitals can spend up to £100 000 per annum on liquid oxygen, so any device that uses lower oxygen flow rates could have significant economic savings for hospitals (eg, nasal cannulae instead of a simple face mask for medium-concentration oxygen).
Medium-concentration masks and nasal cannulae are usually sufficient (target saturation 94–98%) except for patients with known significant COPD who should receive oxygen from a 24% or 28% Venturi mask or 1–2 L/min from nasal cannulae aiming at a saturation range of 88–92%.
Medium-concentration or high-concentration oxygen is normally used (via nasal cannulae, simple face mask or reservoir mask), but particular attention should be given to patients who have hypercapnic respiratory failure when a 24% or 28% Venturi mask or nasal cannulae at a flow rate of 1–2 L/min would be appropriate.
The method of oxygen delivery will depend on the following circumstances:
Expected duration of treatment.
Type of respiratory illness.
Pattern of breathing (high or low respiratory rate and drive).
Need for humidification.
Risk of carbon dioxide retention.
Presence of confusion and its effect on potential compliance.
Nasal cannulae, simple face masks, reservoir masks and Venturi masks should be used where appropriate (see tables 1–4 and charts 1 and 2 in the main guideline). Nasal cannulae at flow rates or 0.5–1.0 L/min are sometimes used as a substitute for Venturi masks in acute or postacute patients with COPD on respiratory wards (adjusting flow as necessary to achieve the desired ABG tensions). This practice requires the use of paediatric flow meters to ensure consistent and finely calibrated oxygen delivery and is not recommended outside specialist units.
Based on the advantages of each delivery system discussed above, the following recommendations are made for delivery of oxygen in medical emergencies. It is likely that additional equipment will be maintained in specialist units, but specialist treatment is outside the scope of the present guideline.
Good practice points (see tables 1–4)
✓ Most hospital patients can be managed with the same delivery device, as in good practice points which follow section 9.8, but a 24% Venturi mask should also be available.
The high-concentration reservoir mask at 15 L/min is the preferred means for delivering high-concentration oxygen to critically ill patients until reliable pulse oximetry monitoring has been established.
Nasal cannulae should be used rather than simple face masks in most situations requiring medium-concentration oxygen therapy. Nasal cannulae are preferred by patients for reasons of comfort and they are less likely to be removed during meals. There is also a cost-saving.
The flow rate from nasal cannulae for medium-concentration oxygen therapy should be adjusted between 2 and 6 L/min to achieve the desired target saturation.
Venturi masks are recommended for patients requiring precise control of FiO2. Venturi masks can deliver a constant FiO2 of 24%, 28%, 31%, 35%, 40% and 60% oxygen with a greater gas flow than a simple face mask. In those at risk of developing hypercapnic respiratory failure with oxygen therapy, the use of Venturi masks may reduce this risk. Furthermore, there is less likelihood of dilution of the oxygen stream by room air if the patient's inspiratory flow rate exceeds the flow rate delivered by the face mask.
For many patients, 24–28% Venturi masks can be substituted with nasal cannulae at low-flow rates (1–2 L/min) to achieve the same target range.
The flow rate from simple face masks should be adjusted between 5 and 10 L/min to achieve the desired target saturation. Flow rates below 5 L/min may cause carbon dioxide rebreathing and increased resistance to inspiration.
Patients with COPD with a respiratory rate of >30 breaths/min should have the flow rate set to above the minimum flow rate specified for the Venturi mask and/or packaging (see figure 11B) (increasing the oxygen flow rate into a Venturi mask increases the total gas flow from the mask but does not increase the concentration of oxygen which is delivered).
HFNC are well tolerated and may be used as an alternative in hypoxic adult patients requiring medium-concentration to high-concentration oxygen therapy and who are not at risk of hypercapnia.
All oxygen delivery systems must have a method of taking the high pressure/flow of gas and reducing it so it can be administered to the patient at a specific flow depending on the individual's needs and mask being used. Piped oxygen points have Schrader flow meters and cylinders have pressure and flow regulators. Most oxygen flow meters use a floating ball to indicate the flow rate. The centre of the ball should be aligned with the appropriate flow rate marking. The example shown in figure 16 indicates the correct setting to deliver 2 L/min.
Flow meter showing correct setting to deliver oxygen at a rate of 2 L/min.
Oxygen tubing is needed to connect flow meters and regulators to the patient delivery device. It is important to ensure that all tubing is connected correctly at both ends. The National Patient Safety Agency has reported frequent adverse events related to oxygen use, including four reports of instances where an oxygen mask was connected in error to a compressed air outlet instead of an oxygen outlet. Compressed air outlets are often used to drive nebulisers in hospitals because they are quieter than electrical compressors. However, the flow meter looks very similar to an oxygen flow meter and is often mounted beside an oxygen flow meter so it is very important to ensure that air flow meters are clearly labelled. There is a similar risk with other piped gas outlets such as those delivering nitrous oxide in some hospitals. Air flow meters are never required in an emergency and should be removed from wall sockets or covered by a designated ‘hood’ when not in use, an example is shown in figure 17.
Air outlet cover.
The guideline authors are also aware of some cases where twin oxygen outlets were in use and the wrong one had been turned on or off. For example, one patient tried to turn off the oxygen flow after finishing a nebulised treatment but accidentally turned off the oxygen flow to a neighbouring patient with serious consequences. It is recommended that patients should not be allowed to adjust oxygen flow, especially if there are dual outlets.
Healthcare organisations should take measures to eliminate the risk of oxygen tubing being connected to the incorrect wall oxygen outlet or to outlets that deliver compressed air or other gases instead of oxygen. Air flow meters should be removed from the wall sockets or covered with a designated air outlet cover when not in use. Special care should be taken if twin oxygen outlets are in use (see recommendation V2).
Evidence statement
Matters related to oxygen tubing and equipment and wall outlets are based on expert opinion and manufacturers' advice (evidence level 4).
Recommendation
V2: Healthcare organisations should take measures to eliminate the risk of oxygen tubing being connected to the incorrect wall oxygen outlet or to outlets that deliver compressed air or other gases instead of oxygen. Air flow meters should be removed from the wall sockets or covered with a designated air outlet cover when not in use. Special care should be taken if twin oxygen outlets are in use (grade D).
The upper airway normally warms, moistens and filters inspired gases. When these functions are impaired by a pathological process or when they are bypassed by an artificial airway, it is common practice to provide humidification. The main reason for using humidification, especially with high-flow oxygen, is that it may reduce the sensation of dryness in the upper airways that oxygen can cause. However, in the non-intubated population, there appears to be little scientific evidence of any benefit from humidified oxygen except that single doses of nebulised isotonic saline have been shown to assist sputum clearance and reduce breathlessness in patients with COPD.478 ,479 There is also evidence that humidification, when combined with physiotherapy, can increase sputum clearance in bronchiectasis.480 RCTs of the effects of humidified high-flow oxygen on patient comfort are required. Use of low-flow oxygen through nasal cannulae is well tolerated without the need for humidification.481 HFNC require warmed and humidified oxygen.
Evidence statement
The use of humidified oxygen in acute care is based on expert opinion (evidence level 4).
Recommendations
Q1: Humidification is not required for the delivery of low-flow oxygen (mask or nasal cannulae) or for the short-term use of high-flow oxygen. It is not therefore required in prehospital care. Pending the results of clinical trials, it is reasonable to use humidified oxygen for patients who require high-flow oxygen systems for more than 24 hours or who report upper airway discomfort due to dryness (grade D).
Q2: In the emergency situation, humidified oxygen use can be confined to patients with tracheostomy or an artificial airway although these patients can be managed without humidification for short periods of time (eg, ambulance journeys) (grade D).
Q3: Humidification may also be of benefit to patients with viscous secretions causing difficulty with expectoration. This benefit can be achieved using nebulised normal saline (grade D).
Humidified oxygen is widely administered in hospitals across the UK and this is presumed to alleviate nasal and oral discomfort in the non-intubated patient. Humidification of supplemental oxygen was commonly delivered by bubbling oxygen through either cold or warm sterile water before it reached the patient. However, the effect on patient comfort is negligible.481 ,482 Bubble humidifiers may, however, represent an infection hazard and should not be used.483 There is no evidence of a clinically significant benefit from ‘bubble bottle’ systems but there is an infection risk.
Evidence statement
The advice not to use bubble bottles is based on expert opinion (evidence level 4).
Recommendation
Q4: Bubble bottles which allow a stream of oxygen to bubble through a container of water should not be used because there is no evidence of a clinically significant benefit but there is a risk of infection (grade D).
If humidification is required, it should ideally deliver the inspired gas at a temperature of 32–36° C. Cold water humidifiers are simple and inexpensive but less efficient than a warm water systems (about 50% relative humidity at ambient temperatures). The warm water option is more effective, targeting a relative humidity of 100%, but both systems are thought to be a potential infection control risk. Warm water humidifiers are expensive and mostly confined to ICUs and HDUs and thus outside the scope of this guideline.
Newer humidifying systems are really ‘giant nebulisers’ with a 1 L reservoir of saline or sterile water and an adjustable Venturi device (figure 18). These systems are attached directly to the oxygen flow meter and connected to an aerosol mask via Flex tube. They allow delivery of precise oxygen concentrations of 28%, 35%, 40% and 60% oxygen via their Venturi device. This requires a specific oxygen flow rate as well as adjusting the Venturi nozzle on the device. It is possible to deliver 24% oxygen using a special adaptor. These large volume humidifiers have a high humidification output. The main indication for use is to assist with expectoration of viscous sputum. There are no published randomised studies involving these devices, but it has been shown that single doses of nebulised saline can assist sputum production and relieve breathlessness in patients with COPD.478 ,479
Large volume nebulisation-based humidifier.
Good practice points related to humidified oxygen therapy
Consider use of a large volume oxygen humidifier device for patients requiring high-flow rates or longer term oxygen, especially if sputum retention is a clinical problem.
In the absence of an artificial airway, the decision to humidify supplemental oxygen needs to be made on an individual basis but this practice is not evidence-based.
The number of patients with a tracheostomy being cared for in a ward setting is increasing as critical care personnel use this as a method of facilitating weaning from mechanical ventilation. In the absence of a pressurised circuit, oxygen is predominantly delivered via tracheostomy mask. This is a variable performance device and delivers concentrations up to 60–70%. If the patient deteriorates and requires an increased oxygen concentration exceeding the concentration that a variable performance interface can deliver (60–70%), it will be necessary to seek an alternative delivery system, usually a T-piece device fitted directly to the tracheostomy tube.
With a mask system, the interface will be connected to a humidification system via elephant tubing. As inserting a tracheostomy tube bypasses the patient's natural mechanisms to warm and moisturise inspired gases, it is essential to humidify any supplemental oxygen being delivered to the tracheotomised patient. This will help maintain a patent tracheostomy tube, reducing the build-up of secretions within the inner tube or the tracheostomy itself and minimising any subjective discomfort that the patient may experience.
Evidence statement
The use of tracheostomy masks is based on expert opinion and clinical experience (evidence level 4).
Recommendation
P1: When oxygen is required by patients with prior tracheostomy or laryngectomy, a tracheostomy mask (varying the flow as necessary) should achieve the desired oxygen saturation (tables 1–4). An alternative delivery device, usually a T-piece device fitted directly to the tracheostomy tube, may be necessary if the patient deteriorates (grade D).
In patients with acute severe asthma, oxygen should be used as the driving gas for the nebulised bronchodilators whenever possible at a gas flow rate of 6–8 L/min because these patients are at risk of hypoxaemia. If the available cylinders in general practice do not produce this flow rate, an air-driven nebuliser (with electrical compressor) should be used with supplemental oxygen by nasal cannulae at 2–6 L/min to maintain an appropriate oxygen saturation level. There is some evidence that bronchodilator therapy (whether delivered by nebuliser or by metered dose inhaler) may cause pulmonary vasodilation leading to increased V/Q mismatch and reduced blood oxygen levels in acutely ill patients and in patients with stable COPD and asthma.484–486 The lowest oxygen saturation occurs not during bronchodilator therapy but about 25 min later.486 One group reported a rise in oxygen saturation during bronchodilator therapy.487
There is some evidence that bronchodilator therapy, however given, can cause increased V/Q mismatch and reduced blood oxygen levels in acutely ill patients shortly after treatment.
When an oxygen-driven nebuliser is given to patients with COPD there is a risk of hypercapnia and acidosis due to the high FiO2 which is delivered. In AECOPD the carbon dioxide level can rise substantially within 15 min of starting high-concentration oxygen therapy.48 Edwards et al488 have confirmed that oxygen-driven nebulisers cause elevation of the blood CO2 level in patients with COPD. The Austin et al's51 study which demonstrated improved mortality with targeted oxygen therapy in patients with AECOPD used air-driven nebulisers to ensure that the target saturation was maintained. When nebulised bronchodilators are given to hypercapnic patients, they should ideally be given using an electrical compressor or ultrasonic nebuliser and, if necessary, supplementary oxygen should be given concurrently by using nasal cannulae at 1–4 L/min to maintain an oxygen saturation of 88–92%. For hypercapnic patients or those with a history of hypercapnia, oxygen saturation should be monitored continuously during nebulised treatments. If an electrical compressor or ultrasonic nebuliser is not available, compressed air can be used to drive the nebuliser but care should be taken to ensure that the nebuliser is not attached to an oxygen outlet (see section 10.8). Once the nebulised treatment is completed, targeted oxygen therapy should be reinstituted.
Compressed air is not routinely available for treatment by ambulance staff. In this situation, oxygen-driven nebulisers may be used but should be limited to 6 min for patients with known COPD because the nebuliser mask delivers a high concentration of oxygen (about 60%). Since most of the effective dose from a nebuliser chamber is delivered within 6 min, limiting oxygen-driven nebulisers to 6 min will minimise the risk of hypercapnic respiratory failure while delivering most of the nebulised drug dose. It must be recognised that patients with COPD may develop hypercapnia and respiratory acidosis if they are left on high-flow oxygen via a nebuliser mask system long after the nebulisation process has finished.
Evidence statement
High-concentration oxygen therapy can cause hypercapnia within 15 min in acute COPD (evidence level 4).
The use of oxygen to drive nebulisers is based on expert opinion and extrapolation from observational studies (evidence level 4).
Recommendations
R1: For patients with asthma, nebulisers should be driven by piped oxygen or from an oxygen cylinder fitted with a high-flow regulator capable of delivering a flow rate of >6 L/min. The patient should be changed back to his/her usual oxygen mask or cannulae when nebuliser therapy is complete. If the cylinder does not produce this flow rate, an air-driven nebuliser (with electrical compressor) should be used with supplemental oxygen by nasal cannulae at 2–6 L/min to maintain an appropriate oxygen saturation level (grade D).
R2: When nebulised bronchodilators are given to patients with hypercapnic acidosis, they should be given using an ultrasonic nebuliser or else a jet nebuliser driven by compressed air and, if necessary, supplementary oxygen should be given concurrently by nasal cannulae to maintain an oxygen saturation of 88–92%. The same precautions should be applied to patients who are at risk of hypercapnic respiratory failure prior to the availability of blood gas results and the oxygen saturation should be monitored continuously during treatment. Once the nebulised treatment is completed for patients at risk of hypercapnic respiratory failure, their previous targeted oxygen therapy should be reinstituted (grade D).
Good practice points
Do not allow hypoxaemia to occur while administering nebulised treatments:
For hypoxaemic patients, oxygen therapy should continue during nebulised treatments.
Driving gas for nebulised treatment in ambulances:
During treatment by ambulance staff oxygen-driven nebulisers should be used for patients with asthma and may be used for patients with COPD in the absence of an air-driven compressor system. If oxygen is used for patients with known COPD, its use should be limited to 6 min. This will deliver most of the nebulised drug dose but limit the risk of hypercapnic respiratory failure (section 10.4). Ambulance services are encouraged to explore the feasibility of introducing battery-powered, air-driven nebulisers or portable ultrasonic nebulisers.
The use of helium–oxygen mixtures is discussed in section 8.18. The evidence base for the use of this gas mixture is weak and the use of Heliox as an inspired gas or as the driving gas for nebuliser therapy is not recommended outside of randomised clinical trials. The use of Heliox affects the delivery of aerosolised treatment in complex ways so the choice of nebuliser systems for the use of Heliox as a driving gas in clinical trials is outside the scope of this guideline. The most likely use for Heliox in clinical practice is for patients with mechanical upper airway obstruction or postoperative stridor. It has been shown that Heliox administration via a standard high-concentration reservoir mask leads to significant dilution by room air.489 For this reason, Heliox should be administered via a system that achieves a gas tight seal, with no leaks between the delivery device and the surroundings.
Heliox 80:20 mixture has a similar oxygen content to air (nitrogen:oxygen 79:21). Heliox 70:30 delivers a higher FiO2 but is more dense than Heliox 80:20 because it contains more oxygen which is denser than helium. The overall balance between oxygen content and gas density has not been addressed in clinical trials but it is recommended that clinicians should aim to keep the saturation in the appropriate target range for the individual patient, usually 94–98% for patients with asthma or upper airway obstruction and 88–92% for patients with severe COPD.
The use of nitrous oxide/oxygen mixtures (Entonox, a 50:50 mix) is discussed in section 8.18. The gas is supplied in a range of cylinder sizes ranging from small portable cylinders for ambulances to much larger ones that can allow the gas to be piped to various outlets around a labour ward. The gas mixture is usually self-administered using a facemask with a demand valve that the patient holds to their face. The demand valve opens to allow gas to flow when it detects an inspiration. Like oxygen, Entonox is classified as a medical gas, and although it is recommended that it is prescribed, it is not a prescription-only medicine. The manufacturers recommend that it should only be prescribed and administered by suitably trained personnel within established clinical guidelines or protocols.
Reduction in oxygen saturation is common during endoscopic procedures that may partially occlude the airway such as bronchoscopy and upper GI endoscopy, and supplemental oxygen is recommended in some guidelines for all patients given sedation and selected patients without sedation.402 ,490 ,491 This guideline emphasises the importance of monitoring oxygenation during the procedure by use of continuous pulse oximetry (see section 8.16).
All guidelines stress caution with the use of sedation and supplemental oxygen in those at risk of hypercapnia. The BSG guidelines recommend preoxygenation at 2 L/min to prevent hypoxaemia, claiming that this is safe even in patients with COPD.491 However, the authors of this guideline recommend that oxygen should be administered only to correct hypoxaemia. Particular caution is advised in patients who may be prone to carbon dioxide retention and the use of transcutaneous CO2 monitoring in these patients has been suggested.492
Generally, oxygen is delivered at a flow rate of at least 2 L/min via nasal cannulae through one or both nostrils to maintain oxygen saturations above 90% or to correct falls in saturation of >4% as discussed in section 8.16. Patient positioning (supine or semirecumbent) had no significant effect on oxygen saturations during bronchoscopy in a study of 38 patients.393
Evidence statement
The use of oxygen during endoscopic procedures is based on expert opinion and extrapolation from observational studies (evidence level 4).
Recommendations J2–J6
J2: All procedures involving conscious sedation warrant routine continuous monitoring of oxygen saturation via pulse oximetry prior to and during the procedure, and in the recovery period, particularly fibre-optic bronchoscopy and upper GI endoscopy where a reduction in SaO2 is common, particularly with concurrent use of sedation.
J3: Significant arterial oxygen desaturation (SpO2<90% or fall of 4% or more that is prolonged (>1 min during endoscopy procedures)) should be corrected by supplemental oxygen with the aim of achieving target oxygen saturations of 94–98%, or 88–92% in those at risk of hypercapnic respiratory failure.
J4: Complicated upper GI endoscopy or procedures in patients with cardiorespiratory comorbidity are especially likely to lead to hypoxaemia and may also lead to hypercapnia, especially if the patient is heavily sedated. It is recommended that blood gases should be measured if such patients should require prolonged oxygen administration. The routine administration of oxygen is not recommended as it may delay the recognition of respiratory failure.
J5: Constant clinical assessment of the patient is crucial at all stages of conscious sedation procedures and monitoring of capnography or transcutaneous carbon dioxide levels may be a useful adjunct to identify early respiratory depression.
J6: During the recovery period after procedures requiring conscious sedation, supplemental oxygen should be titrated to achieve target saturations of 94–98% in most patients and 88–92% in those at risk of hypercapnic respiratory failure (see section 10.5.1).
CPAP is a form of non-invasive ventilatory support that may be used when high inspired oxygen concentrations (>60%) are not sufficient to maintain adequate oxygenation in patients with respiratory failure without hypercapnia. CPAP maintains a fairly constant positive pressure throughout inspiration and expiration, and the positive pressure applied is thought to improve lung expansion, recruit atelectactic areas and offset intrinsic PEEP, reducing work of breathing. Conditions in which CPAP has been used successfully in the management of acute respiratory failure include heart failure, pneumonia, ARDS, chest wall trauma and pulmonary fibrosis avoiding intubation and mechanical ventilation.
The indications, use and equipment required for CPAP are more fully described in the BTS guideline for NIV.209 Generally, a gas flow generator is required, usually powered by the wall air and oxygen supplies or oxygen cylinder, and delivered by a tightly fitting facial or nasal mask, or hood. The level of positive pressure can be adjusted by the use of different sized valves fitted to the mask, or by a single variable valve. Domiciliary CPAP machines used for the treatment of OSA are not suitable for the management of respiratory failure as they may not be able to maintain pressure in patients with rapid respiratory rates and high minute ventilation. Non-invasive ventilators that are designed to deliver BiPAP can be used to deliver CPAP by setting the same inspiratory and expiratory pressure.
Medical oxygen is a drug. However, the legal status of oxygen in the UK is that of a medicinal product on the General Sales List (Medicines and Healthcare Products Regulatory Agency, personal communication). This means that the sale or dispensation of oxygen does not technically require a prescription because it is not a ‘prescription-only medicine’. This status was conferred for practical reasons to facilitate the use of oxygen in the domiciliary setting where the distribution system no longer involves pharmacies. However, the use of oxygen by paramedics, registered nurses, doctors, physiotherapists and others in emergency situations is similar to the use of all other medicinal products by these people. Clinical governance requires that the intentions of the clinician who initiates oxygen therapy should be communicated clearly to the person who actually administers oxygen to the patient and an accurate record must be kept of exactly what has been given to the patient. In this respect, oxygen is in the same category as paracetamol, aspirin, ibuprofen, antihistamines, antiemetics and many other medicines that do not require a prescription if purchased by a patient for his/her own use but do require accurate documentation if administered by a health professional to a patient. In healthcare settings, all of these medicines are conventionally recorded on a ‘prescription chart’ or ‘drug kardex’ alongside drugs in the ‘prescription-only’ category such as antibiotics.
A hospital ‘prescription chart’ is a document in which doctors and other prescribing clinicians make a list of all drugs and medicinal products required by a patient and where registered nurses and other clinicians make a record of all drugs that have been administered to the patient. In many hospitals, the prescription and documentation of administration are recorded directly into the Electronic Patient Record. These documents are also used by hospital pharmacies to dispense medicines but, for technical reasons, these hospital documents (or the equivalent documents in primary care settings or the Patient Report Form (PRF) or electronic PRF used by the ambulance services) do not have the same legal status as a prescription that is given to a patient to take to a community pharmacist for the purposes of dispensing a medicine. The ‘prescription’ of oxygen in acute healthcare settings is therefore not technically a prescription for two reasons: (1) oxygen is not a prescription-only medicine; and (2) a hospital drug chart is not truly a prescription. The second issue applies to all medicines used in healthcare settings, not just to oxygen. However, the words ‘prescription’ or ‘prescription chart’ are widely used to describe the documents which record the use of medicines in UK hospitals and other healthcare settings. For this reason, the present guideline will use the term ‘prescribe’ and ‘prescription chart’ for all orders for oxygen use. The important issue is that there must be a clear written record of all medicinal products, including oxygen, which are given to a patient by healthcare professionals. Ideally, this document should be prepared at the time when oxygen therapy is started. In emergencies, however, clinicians will treat the patient first and subsequently make written records of all treatments given, including oxygen therapy.
Oxygen is prescribed for hypoxaemic patients to increase PO2 and decrease the work of breathing necessary to maintain a given PaO2 (see section 6). The concentration of oxygen required depends on the condition being treated; an inappropriate concentration may have serious or even lethal effects. Appropriate target saturation ranges for common medical emergencies are given in section 8 of this guideline and in tables 1–4. Each hospital should have an agreed policy and protocol for oxygen prescribing to allow staff to adjust oxygen delivery devices and to give oxygen in emergency situations prior to the availability of a prescription. The use of a patient group direction (PGD) may be appropriate if other solutions have not worked in the clinical setting. Please see details at: https://www.nice.org.uk/guidance/MPG2 and http://www.medicinesresources.nhs.uk/en/Communities/NHS/PGDs/.
Although a PGD is not strictly required for medical gases (because they are not a prescription-only medicine) it is important for every organisation to have a written policy to regulate oxygen use up to time when a prescription is written, for example, for patients arriving by ambulance in the emergency department with oxygen use already initiated by the ambulance service. For some organisations, a PGD may be considered as the best way to address this important issue. BTS audits up to 2015 have shown that only 57% of patients using supplemental oxygen in UK hospitals had a valid prescription or written order. This is a situation that would not be tolerated for any other drug.
Oxygen prescriptions may include initial mode of delivery and flow rate (eg, 4 L/min via nasal cannulae). But the most important aspect of the prescription is to give a target range. The clinicians who administer oxygen (usually registered nurses, midwives or physiotherapists) should be trained and empowered to adjust the oxygen concentration upwards and downwards as necessary to maintain the patient in the target saturation range (including adjustments made during nebulised therapy driven by oxygen or nebulised therapy driven by air with simultaneous administration of oxygen by nasal cannulae). This will require all hospitals to have an agreed oxygen administration programme with universal access to educational materials about oxygen administration. The clinicians who monitor the oxygen saturation (often healthcare assistants) should be trained to inform those who have been trained to administer oxygen if the oxygen saturations fall above or below the target saturations. Those doing the monitoring should also understand the importance for the patient of keeping in the target range. Implementing this policy will require all organisations to have agreed procedures (which may include PGDs up to the time when a prescription is written) and training programmes for all clinical staff and regular training programmes in the safe use of oxygen and audit of outcomes.
Many hospitals have developed an ‘admission bundle’ for all patients admitted to hospital. This bundle may include checking for hospital-associated thrombosis risk, checking MRSA risk and the prescription of antithrombotic agents and anti-MRSA agents if appropriate. As part of this process, many hospitals now specify that an oxygen saturation target must be set for all patients on admission to hospital so that the nursing team will know the correct starting target range if oxygen therapy should suddenly become necessary (as well as making a callout to the medical team to assess the patient). Furthermore, this allows nurses making bedside observations to know if the oxygen saturation is appropriate for each patient whether or not the patient is receiving oxygen at the time when the observation is made. Some older people without respiratory problems may have oxygen saturation below 94% and the target range for such patients should be adjusted accordingly. It was reported in the 2011 BTS national emergency oxygen audit that almost half of UK hospitals now have a policy of setting a target saturation range for all patients at the time of admission to hospital. Policies of this sort will become even more important when the EWS system takes oxygen saturation (above or below target range) into account.16
The appropriate device should be used to provide the prescribed oxygen and the effects should be monitored using pulse oximetry, monitoring of respiratory rate and close observation of the patient. Arterial or capillary blood gas analysis should be repeated if clinical progress is not satisfactory and in all cases of hypercapnia and acidosis.
The clinician or registered healthcare professional administering the oxygen therapy should be aware of the hazards of hypoxaemia and hyperoxaemia and the signs and symptoms of inadequate or excessive oxygen delivery.
In the past, oxygen was often not prescribed at all or prescribed on a standard hospital drug chart as ‘oxygen’. It was unusual for the prescription to include full details of what device to use, what flow rate(s) to administer and whether the prescription was for a fixed concentration of oxygen or to aim at a specific oxygen saturation target.4–10
It has been shown that a purpose-designed oxygen prescription sheet can improve oxygen prescribing in the short term, but experience has shown that free-standing oxygen prescription charts are often forgotten and unused.7 Recent audit studies by members of the guideline group (part of annual BTS hospital oxygen audits) have shown improved standards of prescribing with the use of a preprinted section for oxygen use in all hospital drug charts and with prompted electronic prescribing of oxygen for all hospital patients. This system was further enhanced by setting a desired saturation range for each patient. Suggested target saturations for common medical conditions are given in sections 8 and 9 of this guideline. It is important that healthcare professionals where oxygen is administered are familiar with the optimal saturation ranges for common conditions (see online appendix 3), and it is also important that those delivering the oxygen are familiar with the equipment in use and the best types of device to deliver low-concentration, medium-concentration and high-concentration oxygen therapy. Figure 19 shows a working example of a preprinted oxygen section for a hospital prescription chart, and figures 1 and 2 (charts 1 and 2) give advice to prescribers and advice to those delivering oxygen onwards.
The safe use of oxygen includes careful consideration of the appropriate delivery device (mask, cannulae, etc) together with an appropriate source of oxygen and an appropriate oxygen flow rate.
An oxygen target range should be prescribed for all hospital patients. The method and rate of oxygen delivery should be altered by registered nurses or other registered healthcare professionals in order to achieve the prescribed target saturation as per the hospital policy. For most conditions, oxygen should be prescribed to achieve a target saturation of 94–98% (or 88–92% for those at risk of hypercapnic respiratory failure). The nurse should sign this prescription chart or the electronic equivalent on every drug round. This signature on the drug chart confirms that the patient is either receiving appropriate oxygen therapy (the delivery device and flow rate should be documented alongside the SpO2 on the bedside observations chart or electronic observations system) or else has SpO2 within the target range on air at the most recent observation round. It is not necessary to measure oximetry during drug rounds but action may be required if the patient was documented to be outside of their target range at the most recent observations round and if no action has yet taken place.
Evidence statement
Prescription of oxygen in acute illness is based on expert opinion (evidence level 4).
Recommendations for safe prescribing and safe administration of oxygen
S1: Every healthcare facility should have a standard oxygen prescription document or, preferably, a designated oxygen section on all drug-prescribing cards or guided prescription of oxygen in electronic prescribing systems (grade D).
S2: A prescription for oxygen should always be provided, except in sudden illness when it must be started immediately and documented retrospectively (grade D).
S3: Doctors and other prescribers should prescribe oxygen using a target saturation range (sections 8, 9 and 11) and sign the drug chart or electronic prescribing order (grade D).
S4: An oxygen target saturation range should be prescribed for all patients who are admitted to hospital. This will ensure that every patient will receive appropriate oxygen therapy if it should be required. It will also ensure that all clinicians are aware of the appropriate oxygen target range for every patient under their care (grade D).
Good practice points related to prescribing and administering oxygen therapy to patients
Oxygen should be prescribed on the drug chart or electronic prescribing system using a target saturation range.
Oxygen should be prescribed to a target saturation range rather than prescribing a fixed concentration of oxygen or FiO2 (see recommendations A1, A2, A4 and A5).
For hypoxaemic patients, oxygen therapy should continue during other treatments such as nebulised therapy. Clinicians should assess the clinical status of the patient prior to prescribing oxygen and the patient's condition should be reassessed frequently during oxygen use (see recommendations B1–B3).
In most emergency situations, oxygen is given to patients immediately without a formal prescription. The lack of a prescription should never preclude oxygen being given when needed in an emergency situation. However, a subsequent written record must be made of what oxygen therapy has been given to every patient in a similar manner to the recording of all other emergency treatment.
If a patient has an oxygen alert card, initial oxygen therapy should be based on the guidance on the card until the results of blood gases are available.
Monitoring and adjusting therapy (see sections 9–11)
T1: Pulse oximetry must be available in all locations where emergency oxygen is being used by healthcare professionals (see also the limitations of using pulse oximetry section 7.1.2) (grade D).
T2: All documents which record oximetry measurements or blood gas results should state whether the patient is breathing air or a specified oxygen delivery device and flow rate using the abbreviations shown in table 5 (grade D).
T3: In all situations where repeated blood gas measurements are required, they should be measured as soon as possible, usually within 30 min of any treatment change, to determine if the proposed target saturations are appropriate. Consider the use of an indwelling arterial catheter if multiple samples are likely to be required (grade D).
T4: Adjustments should only be made by registered staff who have been trained to administer oxygen. If the oxygen saturation falls below the prespecified range, the concentration of oxygen should be increased; if the saturation rises above this range, the oxygen concentration should be reduced. If the monitoring of oxygen saturation is performed by unregistered staff (eg, healthcare assistants), there must be a clear protocol in place which requires that they should inform staff who are trained to administer oxygen if the oxygen saturation is above or below the target saturation (grade D).
Good practice points related to administration of oxygen therapy
For hypoxaemic patients, oxygen therapy should continue during other treatments such as nebulised therapy. Clinicians should assess the clinical status of the patient prior to prescribing oxygen and the patient's condition should be reassessed frequently during oxygen use (see recommendations B1–B3).
The administering healthcare professional should note the oxygen saturation before stating oxygen therapy whenever possible but never discontinue or delay oxygen therapy for seriously ill patients (see recommendation B2).
The healthcare professional should start oxygen therapy using an appropriate delivery system and flow rate as specified in sections 8– 10 of this guideline. The target oxygen saturation should be documented on the respiratory section of the observation chart.
Whenever possible, patients should be given an oxygen information sheet (example in web appendix 6 of this guideline on the BTS website).
Staff should check the oxygen supply and connections on a regular basis because there have been serious incidents due to disconnection or misconnection of oxygen supplies.
Staff must ensure that adequate oxygen is provided during transfers and while patients are in diagnostic departments. Additionally, oxygen saturation should be monitored continuously for seriously ill patients who require escorted transfers. This is because there have been serious incidents involving accidental discontinuation of oxygen or cylinders running out during interward transfers or transfers to other departments such as for x-rays.
Practical aspects of oxygen dispensing, documentation and monitoring
W1: Registered nurses and others who dispense drugs in hospitals should sign the drug chart or electronic prescribing record at every drug round and check that the patient is receiving oxygen therapy. This is to check that the patient is within the target saturation and also to check whether weaning and discontinuation should be instituted (grade D).
W2: Most patients are prescribed an oxygen target range. If patients are on air at the time of the drug round, registered nurses should sign the drug chart using a code such as ‘A’ for air and the observation chart should also be filled in using the code A for air (see table 5 and figure 19; grade D).
W3: All patients should have their oxygen saturation observed for at least 5 min after starting oxygen therapy or for patients who require an increased concentration of oxygen and after oxygen therapy has been decreased or stopped (grade D).
W4: If the oxygen saturation is above the target saturation range and the patient is stable, the delivery system or oxygen flow rate should be modified to return the saturation to within the target range (grade D).
W5: Patients who have a target saturation of 88–92% should have their blood gases measured within 30–60 min. This is to ensure that the carbon dioxide level is not rising. This recommendation also applies to those who are at risk of developing hypercapnic respiratory failure but who have a normal PCO2 on the initial blood gas measurement (grade D).
W6: Stable patients whose oxygen saturation is within their target saturation range of 94–98% do not need repeat blood gas measurements within 30–60 min if there is no risk of hypercapnic respiratory failure and acidosis and may not need any further blood gas measurements unless there should be further deterioration including symptoms or signs of possible hypercapnia (grade D).
W7: Stable patients on oxygen treatment should have SpO2 and physiological variables (eg, NEWS) measured four times a day (grade D).
W8: In those who have signs of critical illness (eg, NEWS 7 or above), oxygen saturation should be monitored continuously and the patient may require level 2 or 3 care on a HDU or critical care unit (grade D).
W9: If the patient is clinically stable and the oxygen saturation is within the target range, treatment should be continued (or eventually lowered) depending on the clinical situation (grade D).
W10: Oxygen therapy should be increased if the saturation is below the desired range and decreased if the saturation is above the desired range (and eventually discontinued as the patient recovers) (grade D).
W11: The new saturation (and the new delivery system) and flow rate should be recorded on the patient's observation chart after 5 min of treatment at the new oxygen concentration. Each change should be recorded by the clinician trained to administer oxygen by signing the observation chart (only changes should be signed for) (grade D).
W12: Repeat blood gas measurements are not required for stable patients who require a reduced concentration of oxygen (or cessation of oxygen therapy) to maintain the desired target saturation (grade D).
W13: Patients with no risk of hypercapnic respiratory failure do not always need repeat blood gas measurements after an increase in oxygen concentration. However, the patient requires clinical review to determine why the oxygen saturation has fallen (grade D).
W14: Patients at risk of hypercapnic respiratory failure (usually those with a target range of 88–92%; see table 4) require repeat blood gas assessment 30–60 min after an increase in oxygen therapy (to ensure that the carbon dioxide level is not rising) (grade D).
W15: For patients with no risk of hypercapnic respiratory failure, monitoring by pulse oximeter is sufficient (repeated blood gases not required) provided the patient is clinically stable and the oxygen saturation remains in the desired range, usually 94–98% (grade D).
W16: If a patient's oxygen saturation is lower than the prescribed target range, first check all aspects of the oxygen delivery system and the oximeter device for faults or errors (grade D).
W17: If a patient's oxygen saturation is consistently lower than the prescribed target range, there should be a medical review and the oxygen therapy should be increased according to an agreed written protocol (grade D).
W18: If the oxygen saturation fails to rise following 5–10 min of increased oxygen therapy or if there is clinical concern following medical review, then blood gas measurements should be repeated (grade D).
Training in oxygen prescribing and use
X1: All clinicians prescribing oxygen should have appropriate training and access to written or electronic oxygen prescribing guidelines based on this national guideline (grade D).
(Training slides for doctors and nurses are available as online supplementary appendices 7 and 8 on the BTS website.)
X2: Every hospital should have a training programme to ensure that clinical staff are familiar with the hospital's oxygen administration policies. In view of the high number of adverse incidents related to oxygen therapy, it is recommended that all acute Trusts should include basic training in oxygen use in the mandatory training programmes for all clinical staff (grade D).
Safe prescribing and safe administration of oxygen are closely linked. In emergencies, oxygen therapy should be started immediately and documented as soon as possible. In all other situations, oxygen should be prescribed in accordance with the standards described in section 11.1 before administration is started. The healthcare professional who administers the oxygen therapy (usually a nurse or physiotherapist) should be fully trained and should follow local or national protocols as described in section 11.1.
Good practice points
The administering healthcare professional should note the oxygen saturation before starting oxygen therapy (see recommendation B2).
The healthcare professional should start oxygen therapy using an appropriate delivery system and flow rate as specified in sections 8 –10 of this guideline. The target oxygen saturation should be documented on the respiratory section of the observation chart.
Whenever possible, patients should be given an oxygen information sheet (example in web appendix 6 of this guideline on the BTS website).
Pulse oximetry should be available to all healthcare staff managing patients receiving oxygen therapy and they should be trained in their use (see section 7 for technical and practical information regarding oximeter use). Clinicians should be aware that pulse oximetry gives no information about the PCO2 or pH and most pulse oximeters are unreliable when a patient's SpO2 falls below about 85%. Pulse oximetry is dependent on pulsatile flow, and it may not be possible to achieve a satisfactory oximeter reading in patients with cold hands, especially those with severe Raynaud's phenomenon due to collagen vascular diseases (which may also cause hypoxic lung disease). The readings may also be affected by shock, skin pigmentation, nail varnish, etc (see section 7). It is essential to record the oxygen delivery system alongside the oximetry result.
All measurements of oxygen saturation should be recorded in the observation chart along with the code for the oxygen delivery system that is being used. If the patient is breathing air at the time of the observation, this should also be recorded in the chart (see recommendation B2 and figure 19).
Arterial or arterialised capillary blood gases should be measured and the oxygen device and flow rate should be noted on arrival at hospital (or at the time when oxygen therapy becomes necessary) for most patients requiring emergency oxygen therapy (see recommendations C1–C3).
Blood gas measurements should be repeated in all critically ill patients and in many other cases according to the response to treatment (see recommendations C1–C3).
EWS systems such as the NEWS are useful for monitoring patients.
Tachypnoea is a sensitive indicator of deteriorating respiratory function.
All acutely ill patients should have physiological monitoring using EWS or a similar physiological assessment system in addition to pulse oximetry (see recommendation B3).
The original 2012 version of the NEWS allocated inappropriate points for hypoxaemia to patients with target ranges below 94–98% who were within their target range. It was necessary to correct for this when using such charts.165 This is recognised in the 2017 update of the NEWS chart which makes special provision for patients at risk of hypercapnia. Patients at risk of hypercapnia should score no NEWS points for saturation if within their target range and they should score points if the oxygen saturation falls below the target range or if the saturation rises above the target range while breathing oxygen.
Evidence statement
Monitoring of oxygen therapy is based on expert opinion.
All patients should have their oxygen saturation observed for at least 5 min after starting oxygen therapy or for patients who require an increased concentration of oxygen and after oxygen therapy has been decreased or stopped (see recommendation W3) (evidence level 4).
The exact requirements for monitoring will depend on the clinical condition of each patient. Saturations are usually measured after 1 hour of oxygen therapy and then four-hourly. Stable patients should be monitored four times a day. However, critically ill patients will require continuous monitoring of oxygen saturation and other physiological measurements.
In most instances, failure to achieve the desired oxygen saturation is due to the severity of the patient's illness, but it is important to check that the oximeter is correctly placed and functioning normally as well as checking that the oxygen delivery device and the oxygen flow rate are correct. If the oxygen is being delivered from a cylinder, clinicians should check the labelling of the cylinder to ensure that it is an oxygen cylinder and checks should be made to ensure that the cylinder is not empty or near empty.
Most conditions which require supplemental oxygen therapy will improve with treatment and it will then be possible to reduce the amount of oxygen administered to the patient. Improvement will usually be confirmed by observing an improving oxygen saturation and a reduction in the physiological score on the NEWS observation chart as discussed in section 7.
Evidence statement
Adjustment of oxygen therapy is based on expert opinion (evidence level 4).
Recommendations
U1: Lower the oxygen concentration if the patient is clinically stable and the oxygen saturation is above the target range or if it has been in the upper zone of the target range for some time (usually 4–8 hours) (grade D).
U2: If the target saturation is maintained, the new delivery system and flow should be continued. Repeat blood gas measurements are not required. If the patient is stable, the process can be repeated and the patient can eventually be weaned off oxygen (see section 12) (grade D).
In most acute illnesses, oxygen therapy will be reduced gradually as the patient recovers and oxygen therapy can be discontinued once the patient can maintain a saturation of 94–98% while breathing air (or the patient's baseline oxygen saturation level if known). Some patients may have episodic hypoxaemia during recovery from acute illness (eg, patients with COPD with intermittent mucus plugging) and some convalescent patients may be comfortable at rest with a satisfactory oxygen saturation but may desaturate and become breathless when they start to mobilise. The ongoing prescription of a target saturation range will cover both of these types of occurrence.
Some patients with chronic lung diseases will already be established on long-term oxygen therapy and should be tapered slowly to their usual maintenance oxygen delivery device and flow rate.
A small number of patients who have suffered major respiratory or cardiac injury may require a prescription for home oxygen to permit safe discharge from hospital. However, many patients with COPD exacerbations may have a low PO2 on discharge from hospital but a reasonable PO2 at a subsequent clinic visit, so decisions about long-term oxygen should not be made on the basis of blood gas measurements made during AECOPD (see BTS guideline for home oxygen in adults).13
Evidence statement
Reduce oxygen therapy gradually for stable patients (see section 11.3.7). Weaning and discontinuation of oxygen therapy is based on expert opinion in the absence of randomised trials (evidence level 4).
Recommendations
U3: Most stable convalescent patients will eventually be stepped down to 2 L/min via nasal cannulae prior to cessation of oxygen therapy. Patients at risk of hypercapnic respiratory failure may be stepped down to 1 L/min (or occasionally 0.5 L/min) via nasal cannulae or a 24% Venturi mask at 2 L/min as the lowest oxygen concentration prior to cessation of oxygen therapy (grade D).
U4: Oxygen therapy should be stopped once a patient is clinically stable on low-concentration oxygen and the oxygen saturation is within the desired range on two consecutive observations (but the prescription for a target saturation range should remain active in case of future deterioration). It may be appropriate to alter the target range following senior review in patients with chronic cardiopulmonary disease who either have saturations <94% when stable or in whom it is deemed sensible to discharge from hospital with saturations <94% pending an outpatient oxygen assessment. Oxygen should also be stopped if the patient has come to the end of a written protocol of timed oxygen (eg, postoperatively) (grade D).
U5: Oxygen saturation on air should be monitored for 5 min after stopping oxygen therapy. If it remains in the desired range it should be rechecked at 1 hour (grade D).
U6: If the oxygen saturation and physiological ‘track and trigger’ score (eg, NEWS) is satisfactory at 1 hour, the patient has safely discontinued oxygen therapy. However, saturation and physiology should continue to be monitored on a regular basis according to the patient's underlying clinical condition (grade D).
U7: If the saturation falls below the patient's target range on stopping oxygen therapy, restart the lowest concentration that maintained the patient in the target range and monitor for 5 min. If this restores the saturation into the target range, continue oxygen therapy at this level and attempt discontinuation of oxygen therapy again at a later date provided the patient remains clinically stable (grade D).
U8: If a patient requires oxygen therapy to be restarted at a higher concentration than before to maintain the same target saturation range, the patient should have a clinical review to establish the cause for this deterioration (grade D).
U9: Some patients may have episodic hypoxaemia (eg, after minor exertion or due to mucus plugging) after they have safely discontinued oxygen therapy. An ongoing prescription for a target saturation range will allow these patients to receive oxygen as the need arises but transient asymptomatic desaturation does not require correction (grade D).
Audits of oxygen prescription and use have been carried by the BTS in 2008 prior to the launch of the first edition of this guideline and most years since then.16 About 14% of UK hospital patients receive supplemental oxygen therapy on any given day but only one-third of these patients had any type of prescription or written order for oxygen in 2008, this had risen slowly to only 57% by the time of the 2015 audit.493 ,494 Audit of oxygen use within individual healthcare organisations is strongly encouraged and the oxygen champion at each Trust can compare their results with the average for all other units.
It is recommended that all users of oxygen will audit their own practice against the suggested optimal practice suggested in this guideline. This applies especially to high-frequency users such as ambulance services, emergency departments and medical wards.
On the job audit
Regular reviews of the drug card and observation chart on medical rounds at the pilot sites have been very important in the successful introduction of this policy. This has provided instant feedback for doctors, nurses and healthcare assistants and has produced successful change.
Whole hospital and ward audits
An audit tool is available on the BTS audit website (https://audits.brit-thoracic.org.uk/). This has been successfully used UK wide and since 2008 with annual nationwide audits and the facility for individual units to use the audit tool for a local audit at any time. The audit tool allows healthcare organisations to monitor how many patients are receiving oxygen therapy, whether there is a valid prescription and the proportion of patients within the target range. Healthcare organisations can also audit the documentation of oxygen saturation on observation rounds and whether oxygen has been signed for on drug rounds. Organisational issues can also be audited such as the following:
Does the Trust have an oxygen prescribing policy based on this guideline?
Is there a standard prompted oxygen in the prescription document or electronic record?
Is training implemented for nursing staff?
Is training implemented for medical staff?
These matters are covered in more detail in online appendix 11.
Dissemination of this guideline will be encouraged and supported strongly by the societies involved in the production of the guideline.
It is recognised that many healthcare organisations tend to modify national guidelines for local use. Summaries of the guideline for acute hospitals, ambulance services and general practice are shown in online supplementary appendices 3 and 5 on the BTS website (www.brit-thoracic.org.uk). Educational materials are available on the BTS website (appendices 7 and 8). It is hoped that the shortened version of this guideline (or a customised local version) will be made available on the website of every NHS Trust.
It is usual for a new policy to be presented to the local policy committee. A specimen example of a local policy is available in web appendix 4 to help with the production of this policy in individual healthcare organisations.
Implementation of the guideline requires an ‘oxygen section’ in the prescription chart or in the electronic prescribing record in all hospitals. A specimen example is available in figure 19. From experience, it is recommended that oxygen should be placed at the start of the prescription chart because all hospital patients need a specified target saturation range. The oxygen prescription may be missed if it is placed in another part of the drug chart.
Medical staff education is fundamental to the success of this guideline. Teaching slides are available on the BTS website. It is thought that these are suitable for FY1, FY2 and specialty trainees. They are also suitable for undergraduate medical education. Nursing staff and nursing students also require education as do physiotherapists, pharmacists, midwives and other clinicians including healthcare assistants and other unregistered staff who may assist in the care of patients who are using supplemental oxygen. Slide sets have also have also been produced for this purpose and are available on the BTS website. It is suggested that small groups of 5–10 nurses from wards are taught in sessions lasting 30 min each day before the introduction of the guideline locally. This has been found to be more successful than relying on training days as this would take too long to train enough staff adequately.
Local champions exist in hospitals, local champions in hospitals, PCT providers and ambulance services who have helped to introduce these guidelines. The Guideline Development Group are very grateful to the local oxygen champions for organising the introduction of local oxygen policies in 89% of UK acute hospital Trusts by 2011. In most instances, the oxygen champions have introduced a new prescription chart and helped to organise staff education. Clinical governance leads will also need to become committed to the implementation of the Emergency Oxygen Guideline and audit of this process.
One major benefit of nationwide implementation is that, when staff transfer between organisations, they will be familiar with the oxygen prescription and administration system.
Because of the life and death nature of many conditions for which emergency oxygen therapy is used, it seems that clinicians have been wary of conducting controlled trials of oxygen therapy for most of the commoner indications. Additionally, it can be difficult to obtain ethical approval for such studies because seriously ill patients are usually not able to provide informed consent.
Further research is required in many areas including:
Basic physiological studies
Effect of cigarette smoking on blood levels of oxygen and carbon dioxide in acute illness.
Clinical trials
Randomised trial of ‘precautionary use’ of oxygen in critical illness compared with a conservative policy of monitoring carefully and giving titrated oxygen therapy oxygen only if the saturation falls below the target range (and trials to determine the best target range to aim for).
RCTs of nasal high-flow humidified oxygen compared with NIV or high-concentration oxygen in critical illness.
The optimal oxygen target values and their feasibility during CPR and immediately after a restoration of spontaneous circulation in order to improve survival and neurological outcome.
Prospective studies of the effect of oxygen in non-hypoxaemic patients with major trauma and head injury.
Use of oxygen in myocardial infarction (at date of guideline publication, AVOID study is published in 2016 and DETO2X-AMI trial is ongoing).330–333
Use of oxygen in unstable coronary syndromes or type 2 myocardial infarction.
Use of oxygen in chest pain of presumed cardiac origin.
Studies to determine if different types of oxygen mask can affect clinical outcomes.
Use of oxygen in obstetric emergencies.
Prospective studies to determine the optimal target saturation range for patients not at risk of hypercapnia, for example, target range 92–96% vs 94–98%.
Use of nasal cannulae to deliver low-dose oxygen therapy (eg, nasal cannulae at 0.5–1.0 L/min compared with 24% and 28% face masks).
Prospective studies to establish the ideal target saturation range in patients with exacerbated COPD; for example, should the target range be 88–92% or slightly lower or slightly higher for optimal outcome?
RCTs of nasal high-flow (but low concentration) humidified oxygen compared with NIV in patients exacerbated COPD with hypercapnic respiratory failure and pH 7.30–7.35 following initial optimisation of treatment.
RCTs of titrated oxygen therapy in acute presentations of patients with conditions associated with chronic respiratory failure (eg, neuromuscular disease or obesity-associated hypoventilation).
RCTs of titrated oxygen therapy in patients presenting acutely with non-hypercapnic respiratory failure (eg, heart failure, pneumonia).
Randomised trials to determine if nitrous oxide is an effective analgesic agent and if the oxygen component affects clinical outcomes.
Randomised trials to determine if clinical outcomes can be improved by the use of Heliox mixtures and, if so, which conditions are likely to benefit.
Use of oxygen as required for relief or breathlessness in non-hypoxaemic patients with acute illness.
Effects of humidified high-flow oxygen on patient comfort.
Effects of increased flow rates from Venturi masks on patient comfort and oxygen saturation.
Further comparisons of high-flow nasal oxygen with reservoir masks and high-concentration Venturi masks.
Implementation studies
Benefits of alert cards and personalised oxygen masks for patients with prior hypercapnic respiratory failure.
Further studies of clinical outcomes of patients exposed to hyperoxia.
Relationship between oxygen levels and outcomes in a wide range of conditions.
Studies to determine if implementation of this guideline improves patient outcomes.
Studies to determine the best way to help clinicians to comply with guideline recommendations.
Systematic reviews
Outcomes from different levels of oxygen supplementation in AECOPD.
Updated review of oxygen therapy in myocardial infarction.
Review of oxygen therapy in stroke.
Guideline group members, representation and guideline sections
联系客服






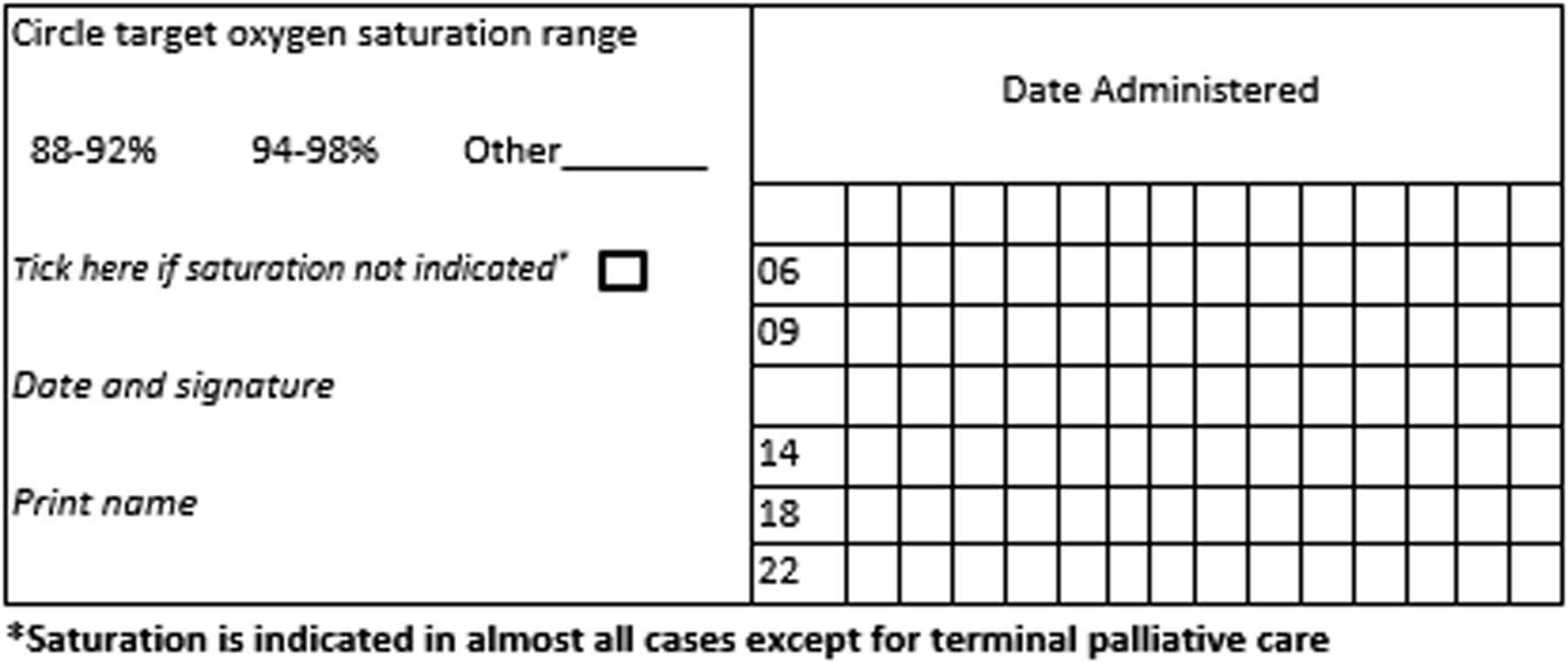


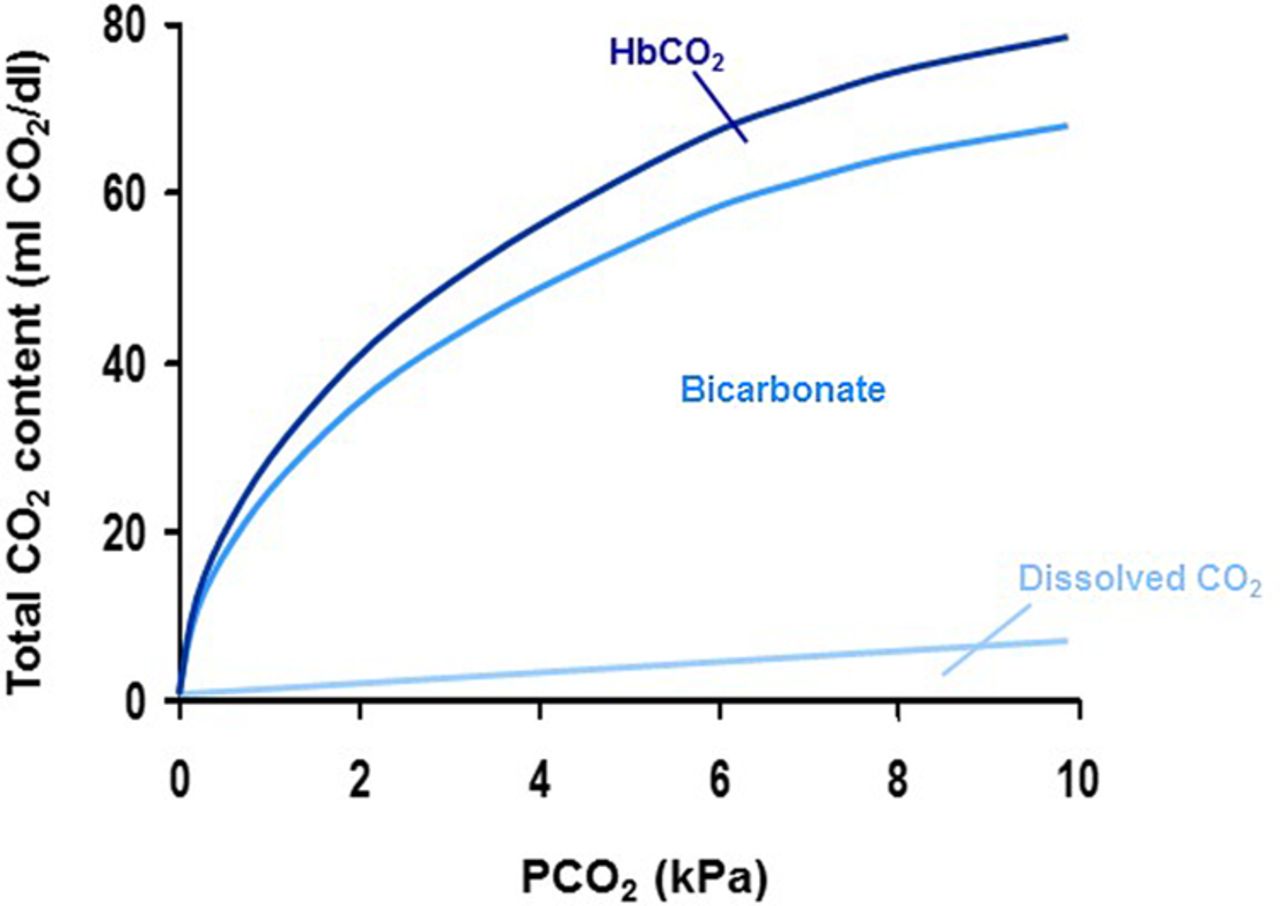


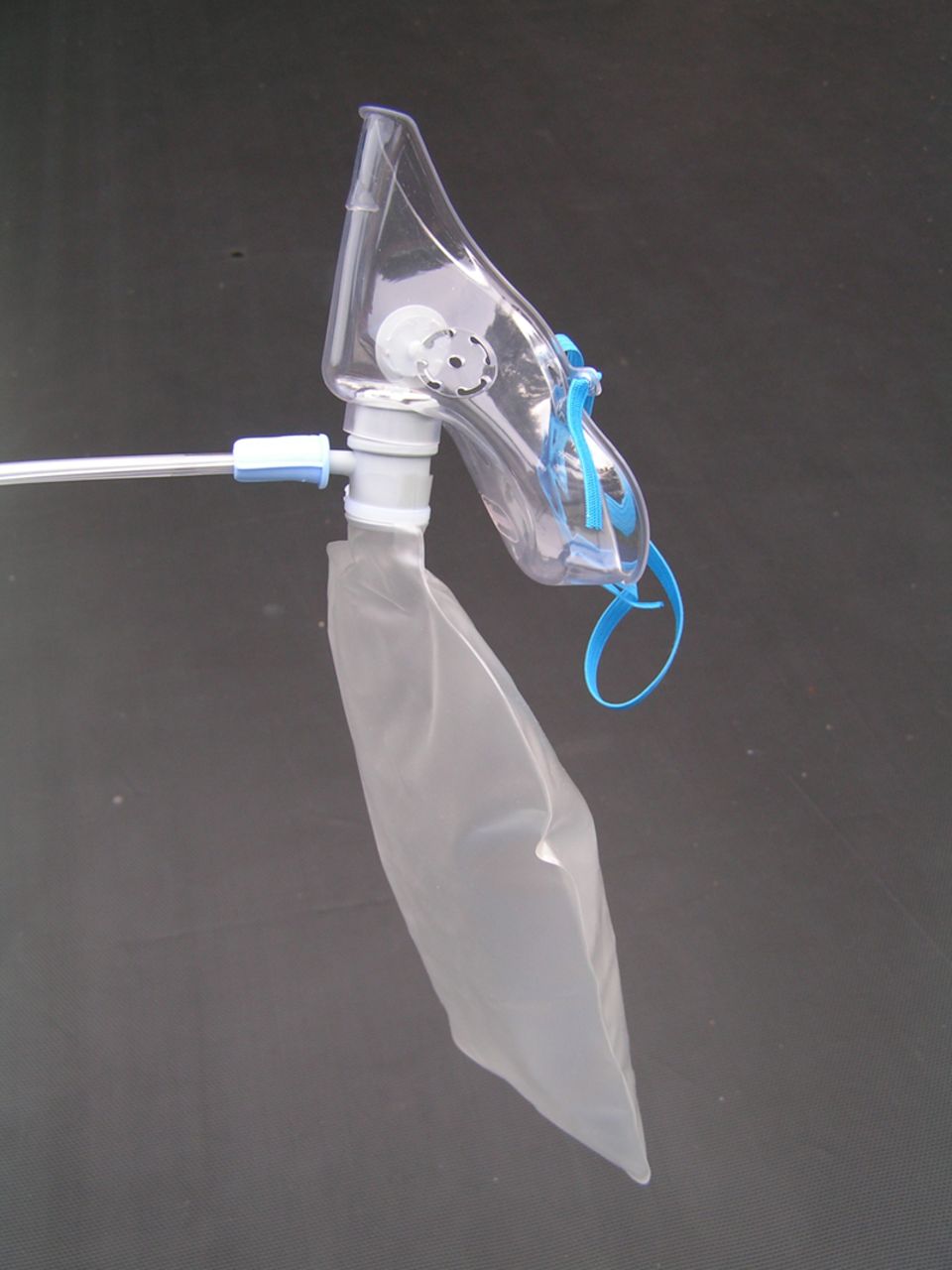




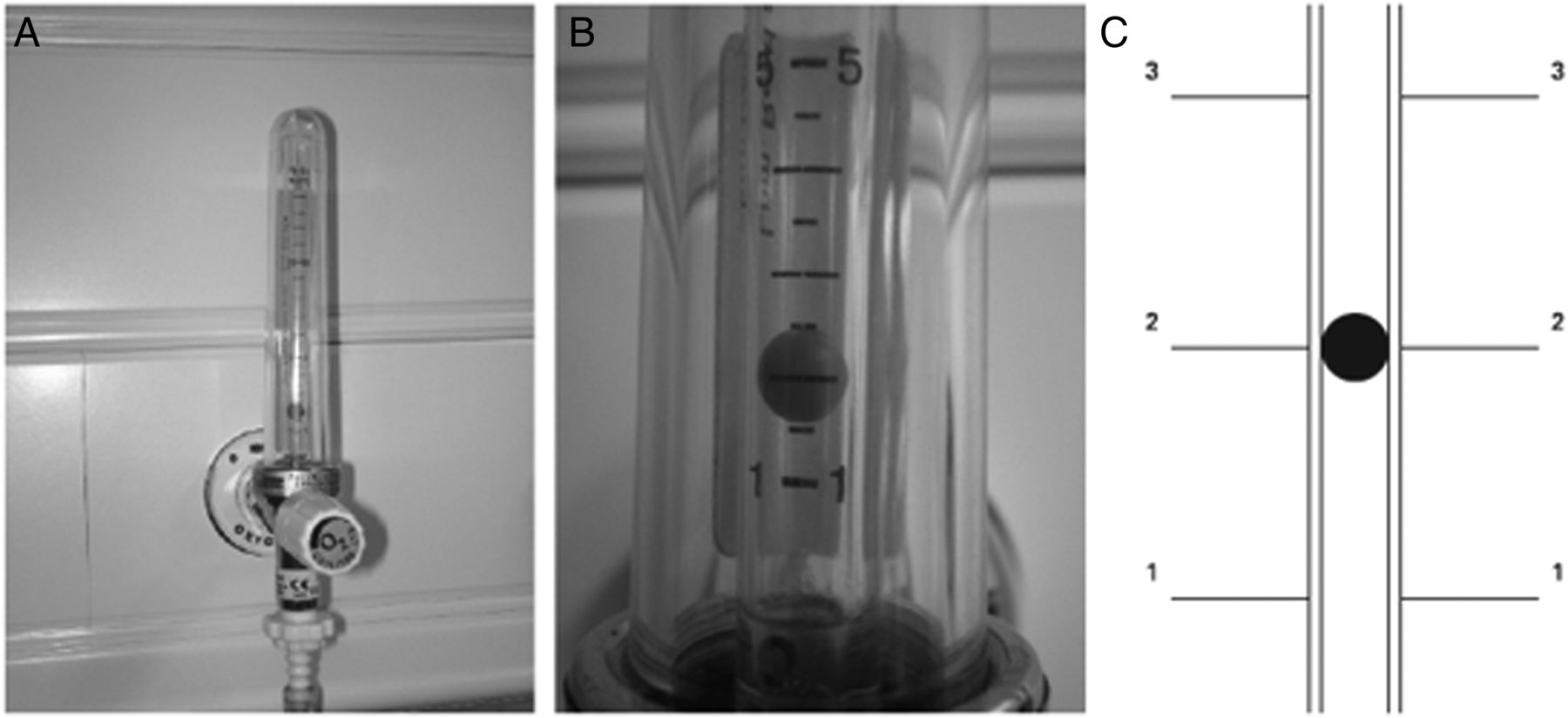



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
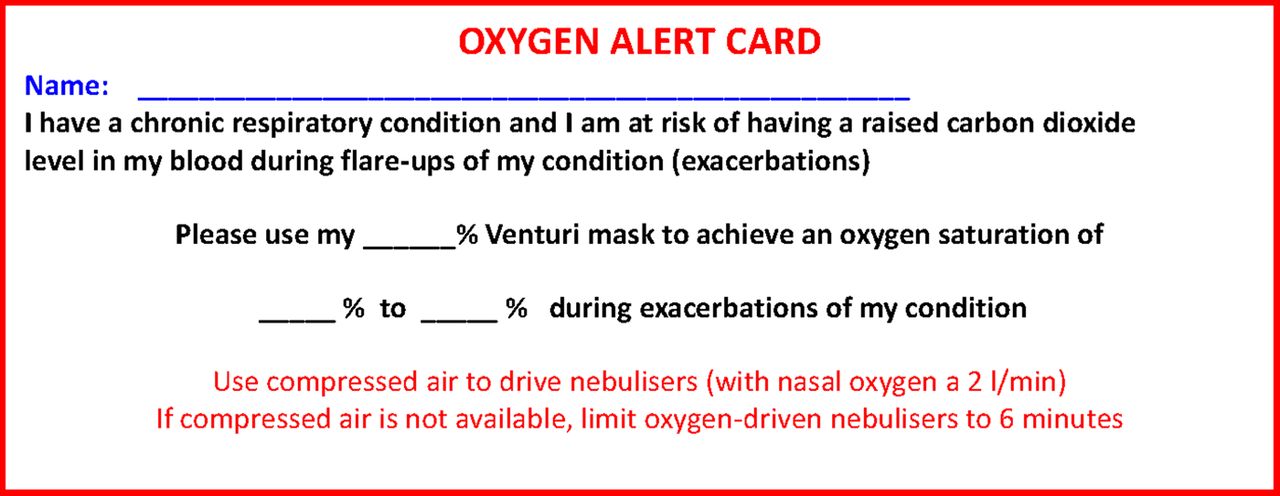{kind=link}
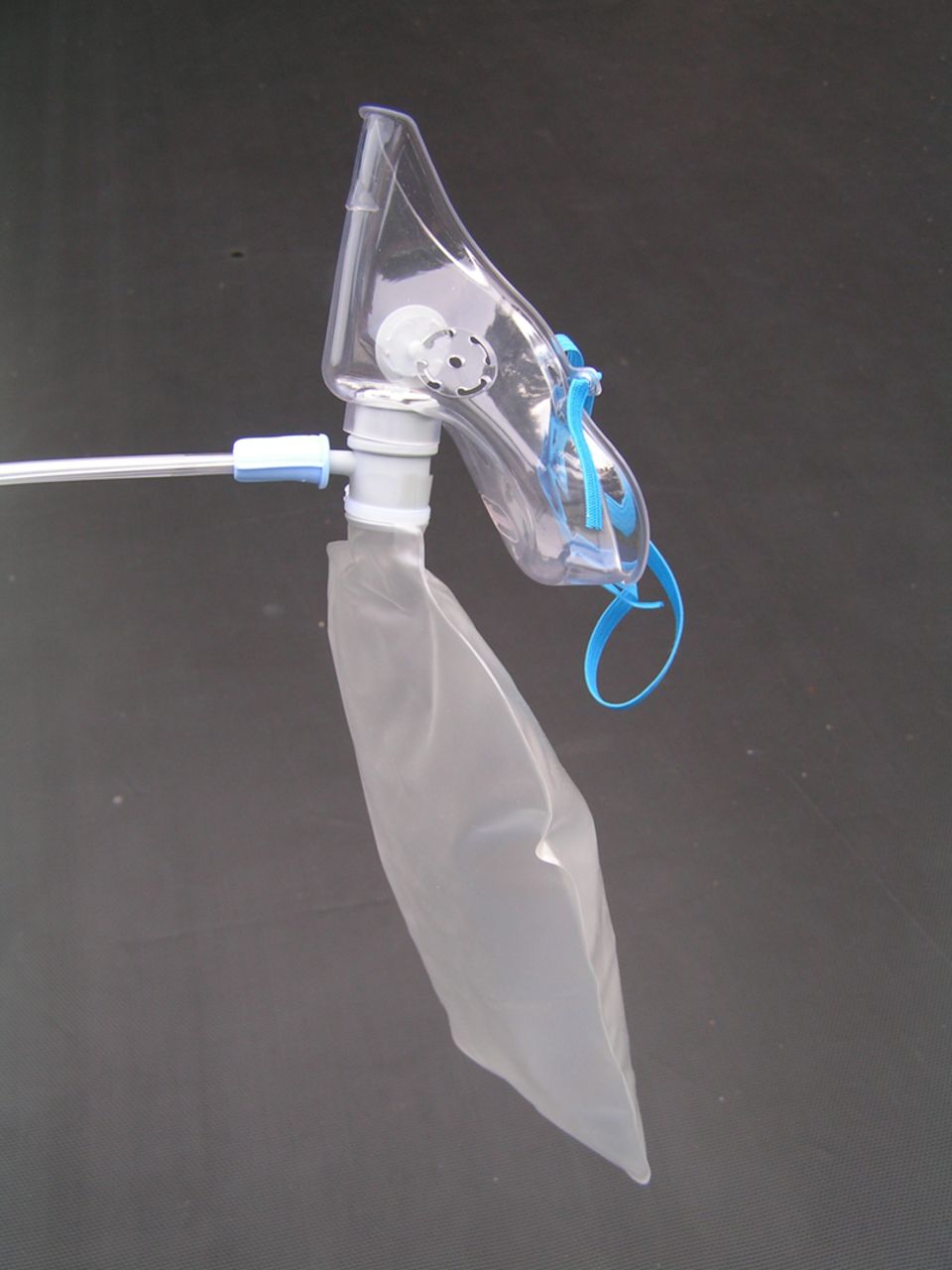{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
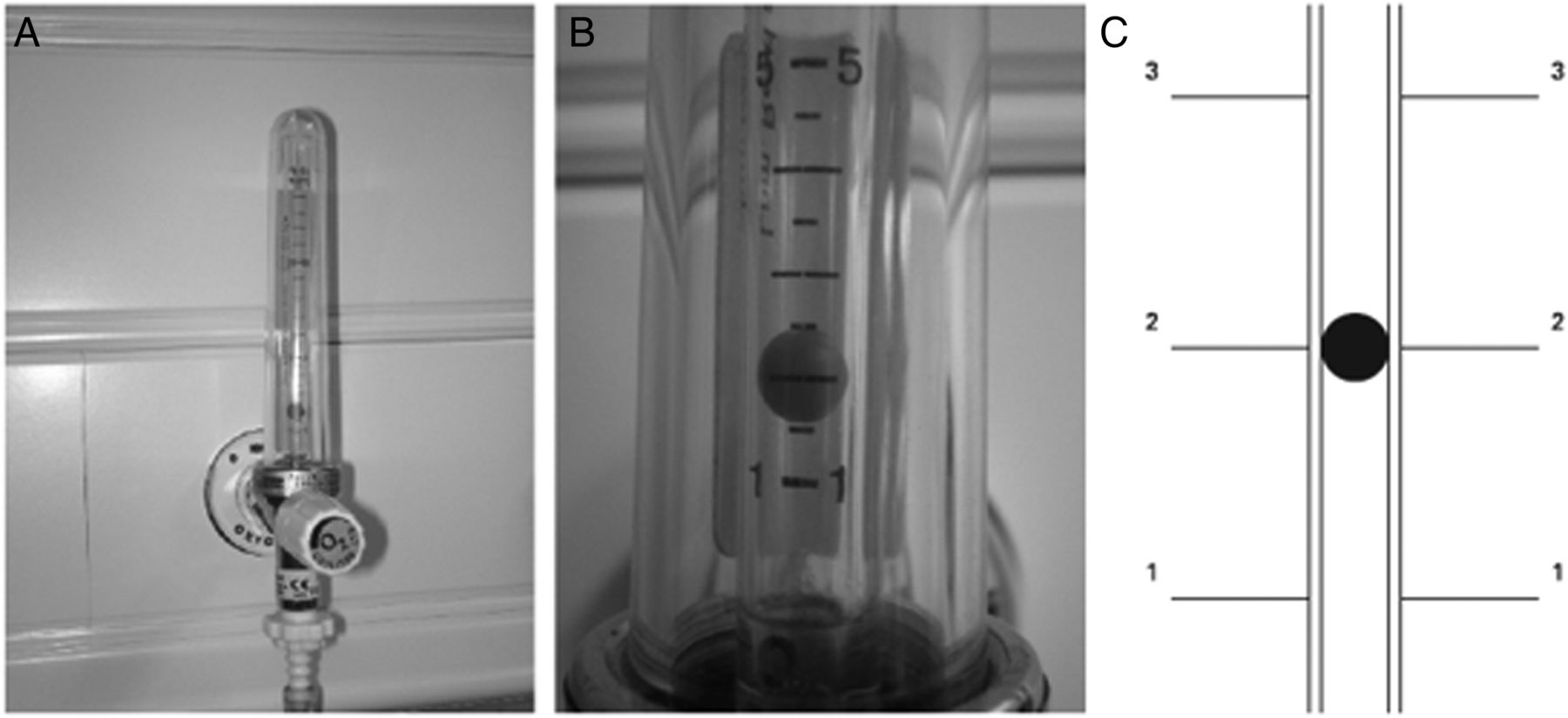{kind=link}
{kind=link}
{kind=link}